Download
1 / 27
270 likes | 275 Vues
HYDROCEPHALUS prof: Dr Arjun Shetty. Hydrocephalus is the increased accumulation of csf in the brain increased production of csf decreased absorption of csf obstruction to the flow of csf. Increased production of csf

E N D
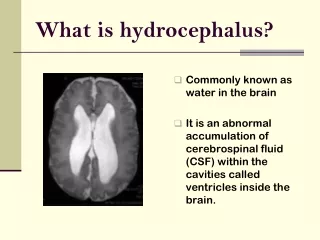
Hydrocephalus is the increased accumulation of csf in the brain • increased production of csf • decreased absorption of csf • obstruction to the flow of csf
Increased production of csf Approximately ml of csf is present in an adult Rate of production of csf is ml per msq body surface area
CSF is produced by an acute process in the choroid plexeus of the lateral ventricles.Passive production also occurs. • The production of csf is not sensitive to changes in ICP however absorption increases with raised ICP • CSF production is maximum at about 2am and minimum at about 6pm (3.5 times)
Factors affecting production: - drugs which decrease blood flow,eg., vasopressin increase - Acetazolamide reduces csf production by uncoupling blood flow from csf production - Glycerol reducess csf production by increasing hyperosmolarity of blood - csf production is less in elderly patients copared to young patients
Over production of csf: - choroid plexeus papilloma - choroid plexeus paapillitis
Impared venous drainage : - csf is absorbed into the supra saggital sinus through the arachnoid granulations - upto a threshold point increase csf is associated with increased absorption of csf - Radical neck dissection ,superior venacava obstruction ,dural sinus thrombosis do not cause an increase in ventricular size in adults.
Obstruction to csf flow : CSF pathway : lateral ventricle I Foramen of Monro I 3rd ventricle I Aqueduct of sylvius I 4th ventricle I Foramen of Luscka and Magendie I Basal cisterns ( sub arachnoid space) I Superior sagital sinus Obstruction to flow : - from externally - from within the pathway
Communicating and Non communicating hydrocephalus Hydrocephalus is considered to be communicating when the obstruction to flow of csf is in the subarachnoid space Non communicating hydrocephalus is when the csf flow is observed within the ventricular pathway itself
Non communicating hydrocephalus Congenital : - aqueduct stenosis - Dandy Walker cyst - congenital cysts,tumors and arteriovenous malformations
Acquired : - Aqueduct stenosis ( acquired ) - inflammation ( ventriculitis) - tumors : choroid cysts, intra and extra ventricular tumors - blood and other non neoplastic lesions
Communicating hydrocephalus congenital : Arnold Chiari malformation Encephaloceles Absence of arachnoid granulations
Acquired - Leptomeningeal inflammation due to infection, blood - Increased csf production due to SOL.
Pathophysiology: 1. atrophy of white matter 2. oedema of brain surrounding the ventricles 3.fibrosis of choroid plexeus 4. stretched ependymal epithelium 5.ventricular diverticula,thinning of intra hemisphere commisures
Acute hydrocephalus - intra ventricular haemorrage - sub arachnoid haemorrhage - head injuries – trans tentorial herniation - shunt obstruction
ventricular dilatation occurs in 3-6 hrs • lateral ventricle dialates first • aqueduct dialates last After 3-6 hrs - ventricular enlargement slows down - ependymal thinning tears- edema, which is maximum by 24 hrs
Chronic hydrocephalus Increase in csf is compensated by : -expansion of skull in infants -reduction of vascular volume - increased ventricular size - cerebral atrophy
Damage to ependymal and choroid plexeus in chronic hydrocephalus reduces csf production • csf flow may be reversed in chronic communicating hydrocephalus
Clinical features : in infants - cranio facial dysproportion - bulging fontanelle - dialated veins of scalp - sunset sign -crack pot sign -unilateral or bilateral 6th nerve palsy - sutural diastasis
In adults : Acute cases- features of raised ICP, transient or sustained blindness,Perinauds syndrome
Chronic cases : - increased ICP - papilloedema and optic atrophy - decreased higher motor functions - 6th nerve palsy - Perinauds syndrome - bitemporal hemianopia - spastic paraperesis with lesser upper limb involvement - endocrine abnormalities: precocious puberty,adiposogenital dystrophy,infantilism
Normal pressure hydrocephalus : - chronic hydrocephlaus with normal csf pressure - small pressure gradient between venticles and brain - associated incomplete csf pathway obstruction
Adults : - dementia - bladder incontinence - ataxia
Children: - increase head size - mild mental retardation - mild spastic paraperesis
Diagnosis : - CT, MRI - iv pressure recording - clinical response to ventricular damage
Arrested hydrocephalus : - csf pressure returns to normal - no ventricle-brain pressure gradient - associated partial obstruction-commonly distal If ventricles are enlarged without central atrophy – shunt could be considered in children