Download

1 / 42
420 likes | 545 Vues
Medical Home and the Community. NFI Grantee Meeting September 18, 2007 Sarah Thorson: Minnesota Department of Health Sharon Fleischfresser: Wisconsin Division of Public Health. Medical Home Breakout Session Outcomes.

E N D
Medical Home and the Community NFI Grantee Meeting September 18, 2007 Sarah Thorson: Minnesota Department of Health Sharon Fleischfresser: Wisconsin Division of Public Health
Medical Home Breakout Session Outcomes • Background information on Medical Home Initiatives in Minnesota and Wisconsin • Share activities of Medical Home implementation in your community • Identify challenges and the Lessons Learned • Explore ideas for Medical Home spread
….We tried a lot of other things first - with sporadic successes • AAP-MN Disability Subgroup Efforts– Title V and Part C funded: Raise awareness of ‘Medical Home’ among pediatricians • Universal Standard Benefit Set • SAFE at Home Partnership: Title V, Family Voices, 2 health plans, individual physicians: to identify CSHCN and to improve the quality of primary care. • Minnesota’s promise: Title V, Family Voices, physician leaders
Then we really started “humming” 2002 Minnesota Medical Home Project: Title V, Family Voices, and AAP-MN, DHS • Assumption we’d all work together • Funds reflected a partnership
The Blueprint: Breakthrough Series(9-12 month time frame) Participants Select Topic Prework P P Develop Framework & Changes D A A D Summits, Guides, Publications, etc. S S Planning Group LS 1 LS 2 LS 3 Supports E-mail Visits Phone Assessments Senior Leader Reports
Group of 11 Primary Care Pediatric Practices & Family Practice Clinics Two parents per team Meet 3 times a year for 2 days of learning and sharing Punctuated with action periods where each team implements MH concepts and improves their Medical Home The Collaborators
Model for Improvement What are we trying to accomplish? How will we know that a change is an improvement? What change can we make that will result in improvement? Act Plan Study Do From: Associates in Process Improvement
Health System Community Health Care Organization (Medical Home) Resources and Policies ClinicalInformationSystems Care Partnership Support DeliverySystem Design Decision Support Timely & efficient Family -centered Evidence-based & safe Coordinated and Equitable Functional and Clinical Outcomes Supportive, Integrated Community Informed, Activated Patient/Family Prepared, Proactive Practice Team
NFI: 21 Teams • Title V priorities (Six core outcomes +SPMs) integrated into curriculum
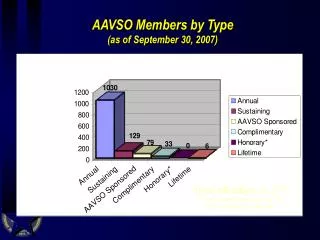
Copy of care plan Visited hospital emergency room in past 3 months Unplanned hospital admission in the past 3 months Family Survey Results
2007 Legislative Session four pilot projects for children and adults with complex health care needs who are enrolled in fee-for-service medical assistance, to the extent permitted by federal requirements. At least two of the grantees must focus on children with autism or children with complex/multi-diagnoses physical conditions. The purpose of the projects is to pilot primary care clinic models of care delivery focused on care coordination and family involvement
2007 Legislative Session (cont) develop and implement a provider-directed care coordination program for medical assistance recipients who are not enrolled in the prepaid medical assistance program and who are receiving services on a fee-for-service basis. This program provides payment to primary care clinics for care coordination for people who have complex and chronic medical conditions. Clinics must meet certain criteria such as the capacity to develop care plans; have a dedicated care coordinator; and have an adequate number of fee-for-service clients, evaluation mechanisms, and quality improvement processes to qualify for reimbursement.
2007 Legislative Session (cont) Of the health care access fund appropriation, $500,000 in fiscal year 2008 and $500,000 in fiscal year 2009 are to expand the medical home learning collaborative initiative in collaboration with the commissioner of human services. Services provided under this funding must support a medical home model for children with special health care needs.
Medical Home - Wisconsin • CSHCN national performance outcome • Participation in the Maternal Child Health Bureau (MCHB)/American Academy of Pediatrics (AAP) Medical Home Mentorship Meeting - January 2002 • Identified as a priority area by the WI MCH/CYSHCN Advisory Committee • National Medical Home Learning Collaborative (NICHQ) • Wisconsin replication in partnership with the Regional CYSHCN Centers • Medical Home for all children as a new WI Title V State Performance Measure
Wisconsin Medical Home Learning Collaborative Utilize rapid QI (Plan, Do, Study, Act) cycles –Small Steps of Change Focus of practice change: • Family Partnerships (focus groups, family surveys, creation of Parent Advisory Committee) • Identification of CYSHCN within the practice • Development of medical care plans (emergency care, care summary) • Linkage to community/state resources
Participating Practices Wisconsin Medical Home Learning Collaborative Regional CSHCN Centers
Medical Home Spread: 2006-2007 • 12 Medical Home local capacity grants (April 2006-Dec 2007) with new cycle January 08 • Medical Home Transitions Learning Collaborative (UW and CHW) - ongoing • Medical Home Summit – 2006 and 2007 • Transition Community Connector grants • Primary Care Practice QI Mini-Grants • Wisconsin Medical Home Toolkit: www.wimedicalhometoolkit.aap.org
Medical Home Practice Sites MH Local Capacity Grants Transition Learning Collaborative Transition Community Connectors Medical Home and Community Grant Sites Regional CYSHCN Centers
Introduce health care providers to Medical Home quality improvement strategies Goals: Simple Steps • Provide a roadmap to tested tools and strategies • Connect providers, their patients and families, to the Regional CYSHCN Centers
Medical Home Strategies: • Engage Patients/Families as Partners • Improve Care Coordination • Create Care Plans • Identification & Screening • Supporting Transitions • Collaborate with Community Resources • Improve Coding and Reimbursement
Wisconsin MH Toolkit Website: Average/Month (March-July2007) • 1419 visitors/month • 316 single visits/month • 179 repeat visits/month • 188 book marked/month • 951 down loads/month • Favorites: care plans, reimbursement/CPT codes
Other Opportunities for Medical Home Spread • Promote spread of MH as QI effort • Link Medical Home LC concepts to long term care reform efforts for children and adults (Family Care) • Child Alert/Preparedness • Wisconsin eHealth Initiative • Other public health programming-adult chronic disease programs • Health care financing-pay for performance
Challenges • MH spread to date is primarily focused at the practice level versus system • Lack of funding/incentives to support care coordination and other MH strategies on a system wide scale • Making the “business case” for MH implementation as a health care delivery model
For More Information • Sarah Thorson: sarah.thorson@health.state.mn.us 651-201-3651 • Sharon Fleischfresser: fleissa@dhfs.state.wi.us 608-266-3674
Discussion • Name an activity that you have been engaged in to support Medical Home implementation in communities in your state? • What are the challenges you’ve encountered? • What strategies have you found to be successful? • Ideas to promote Medical Home Spread in the future?