Download
1 / 29
300 likes | 551 Vues
The significance of Motor Planning, Dominance and VMI. An overview of motor planning with the emphasis on Bilateral Integration & Sequencing, Lateralisation and Visual-Motor Integration Nancy Raubenheimer 25 May 2009. Today’s discussion. What is Praxis / Motor Planning? Components of Praxis

E N D
The significance of Motor Planning, Dominance and VMI An overview of motor planning with the emphasis on Bilateral Integration & Sequencing, Lateralisation and Visual-Motor Integration Nancy Raubenheimer 25 May 2009
Today’s discussion • What is Praxis / Motor Planning? • Components of Praxis • End-products of Praxis • Skills versus “splinter skills” • Types of Praxis difficulties • What is Bilateral Integration and Sequencing? • What is Laterality? • Stages of Lateralisation / Hemisphere Specialisation • What if Lateralisation does not happen? • What should we look out for? • Visual-Motor Integration • Reversals • Questions / Case discussions
What is Praxis / Motor Planning? • Praxis / Motor Planning is a uniquely human skill that enables us to interact effectively with the physical world. Praxis is not just a skill performance. It is an adaptive response (interactive) function. • “It is the ability to conceive of, organise and carry out a sequence of unfamiliar actions.” • “Praxis is the neurological process by which cognition directs motor actions; motor or action planning is that intermediary process which bridges ideation (having an idea) and motor execution (doing it) to enable adaptive interactions with the outside world.” • Praxis is a cortical/cognitive process • The foundations of praxis are sub-cortical • Praxis is a continuum: it changes all the time. You never do the same thing the same way twice. The environment constantly changes
Motor Planning “Postural reactions, centrally programmed movements and learned motor skills do not take much attention or volition; it is enough merely to have a general goal in mind. Motor planning, on the other hand, requires attention. Attention enables the brain to plan the kind of messages to send to the muscles and the sequence in which to send them. An infant motor plans picking up a rattle, putting a spoon into his mouth and crawling through a doorway – until these become skills and no longer require planning. The young child motor plans putting on clothes, writing the alphabet and speaking complete sentences. Learning to use a new tool – even a crayon or a knife – require motor planning. An adult motor plans when he ties an unfamiliar knot, does a new dance step or learns a new job at work. Motor planning is, in some ways, the highest and most complex form of functioning in children. Because it involves conscious attention, it is closely linked to mental and intellectual functions. It depends upon very complex sensory integration throughout the brain stem and cerebral hemispheres. The brain tells the muscles what to do, but the sensations from the body enable the brain to do the telling. Motor planning is the bridge between the sensory-motor and the intellectual aspects of brain function.”
The components of Praxis • Ideation • Motor Planning • Execution / Motor Coordination • Feedback
1. Ideation • (Creativity is not ideation) • Conceptualising the meaning of what something is • Cortical process • Involves language and perception • Functional outcomes: • Recognise and act on problems/situations • Generate ideas / goals for motor action • Intervention Approach: “top-down”
2. Motor Planning • Organisation of self • Putting a sequence in the right order • Feed-forward process: ability to pre-plan an activity • Primary systems involved: tactile, proprioception, vestibular, visual • Expected adaptive response: • Familiar > unfamiliar > complex plans • Intervention approach: “bottom-up”
3. Execution / Motor Coordination • Internal feedback • Awareness of what your body did • Self-perception of movement • Involves vestibular / proprioception / visual integration • Functional outcome: Bilateral coordination and projected action sequences
4. Feedback • Internal and external feedback • Involves all sensory inputs • Functional outcome: lays down motor engrams (stored patterns of familiar motor actions) • Expected adaptive response: production of adapted body actions
End-products of Praxis components • Praxis involves language, cognition and all sensory inputs • Expected adaptive response: complex plans in future • Praxis provides mechanism for organisation of motor performance but also is a necessary foundation for the function of problem-solving and organisation and performance of larger sequences of activities, routines and occupations of daily life • Problem solving has its roots in ability to adapt to environmental demands, which is the cornerstone of praxis • Problems with motor performance have consistently been associated with difficulties in play skills, activities of daily living and social participation as well as having a long-term impact on a wide variety of other areas of function.
Skills versus splinter skills “We use motor planning to learn new things such as getting dressed, until these activities become skills and no longer require planning” • “A skill is something that we initially had to motor plan in order to learn but that we can now do spontaneously” • “Splinter skills” are the skills we learn in the absence of the appropriate foundational skills, or to compensate for inadequate motor planning skills
What are “splinter skills”? “Although a child may not have developed that foundations for a function, society still demands that he perform that function. Therefore, as the child with sensory integrative dysfunction grows older, he learns “splinter skills” that compensate for his poor sensory processing. An example of a splinter skill is the ability to play a particular piece on the piano without having the generalised ability to play the piano. If a child cannot learn to tie his shoelaces through the natural interaction of sensory information in his brain, he will have to learn to tie the knot as a splinter skill. Natural learning through sensory integration is easier, and each learning experience helps the brain learn many other things. Learning a splinter skill takes a lot of effort and concentration and does not help the child in other areas of his life. However, many splinter skills are worth having for their own sake. If a child with sensory integrative dysfunction is bright, he will learn many splinter skills and appear to have typical physical, mental and social functions, but life and just “being” will not be the same as they are for those with adequate sensory integration. With understanding and supportive parents, the child will often lead a gratifying life and carry his share of society’s responsibilities. However, if the stresses of life are too much for his brain’s coping abilities, he may have difficulty keeping up with the ever-increasing demands of daily life.”
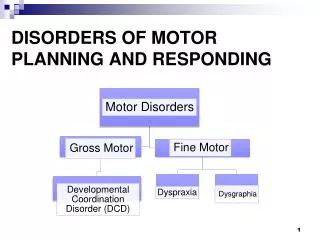
Types of Praxis difficulties • Developmental Coordination Disorder (DCD) • Motor impairment is greater than IQ ability (usually normal IQ) with functional impairment • Characterised by poor coordination and clumsiness • Dyspraxia • An impairment or immaturity in the way the brain processes information, which results in messages not being properly or fully transmitted. • Associated with problems of perception, language and thought • General dyspraxia • Dysfunction in discrimination of tactile and vestibular inputs with performance problems in motor planning and sequencing
Types of Praxis difficulties (cont.) • Somato-dyspraxia • Characterised by decreased tactile (and proprioceptive) discrimination and motor planning problems. • This is conceptualised as a specific problem in the motor planning component of praxis and is manifested in difficulties performing actions such as imitating gestures as well as performing various motor tasks • Bilateral Integration and sequencing dysfunctions • Characterised by primary deficits in vestibular (movement), proprioceptive (muscle and joint), and visual integration deficits. Deficits in this area are reflected in problems with timing, motor coordination, execution and completing projected action sequences. • Dyspraxia of speech • A developmental disability characterised by difficulty in muscle control, specifically in the muscles involved in producing speech. • Also known as Developmental Apraxia of Speech. This is a speech disorder that interferes with a child’s ability to correctly pronounce sounds, syllables and words.
What is Bilateral Integration? • The integration / connection / communication between the bilateral brain hemispheres • This results is the ability to use two sides of the body together in a coordinated manner. The ability to use the lead and assist hands together effectively results in bilateral motor coordination. • Vestibular (movement) and Proprioceptive (joint-and-muscle) systems hold the key for Bilateral Integration • In other words: Bilateral Integration relies on the adequate processing and integration of movement and muscle-joint input
What is Sequencing? • “Projected action sequences”: • the ability to plan and initiate effective movements in response to events that are changing or have not yet happened (to future events in the environment) and to adjust actions to meet future conditions. • This is also called the “feed-forward mechanism” • “Bilateral integration and sequencing” is a disorder of praxis / motor planning
What is Laterality • “Laterality is the internal awareness of the two sides of the body and of their difference.” LeFerure, 1975 • Laterality emerges from the operational organisation of the two sides of the body, including the two brain hemispheres, and which would manifest itself as the completion of a process called “lateralisation”. • Lateralisation can also be called hemisphere specialisation • There are four major stages of lateralisation
Stages of Lateralisation • Mono-lateralisation: from birth – 3 months • The two sides of the body (brain included) would function independently, one from the other, in such a way that the experiences lived by one side would not be sensed by the other • Duo-lateralisation: third month – 12th month • Then child now live the same experiences with both sides either simultaneously or in a rapid alternation for a complete integration • Bi-lateralisation: roughly from 12th month – 24th month • The child would reach this level of integration by setting active relations that will become more and more intricate between him paired limbs and within his basic biological, perceptual-motor and cognitive functions • Integrated lateralisation: from about the 24th month • The proper organisation of this stage would bring about the efficient use of the total body (brain included), stemming from the adequate assimilation of stimuli from the outside world. The adequate accommodation to the stimulations through proper reactions, and the adequate adaptation as a result of the equilibrium between past and present experiences and allowing from anticipation of the future.
What if lateralisation does not happen? • Hemisphere specialisation does not happen • Child develops similar skills with each hand and each cerebral hemisphere • Instead of using just one hand for fine motor work such as writing or using tools, child tends to use right hand on right side of body, and left on left • May be considered “ambidextrous”, but actually not especially skilled with either hand • Or, he might become left-handed while genetically he is meant to be right-handed • Meanwhile, inside the brain, both cerebral hemispheres are doing similar things instead of specialising for greater overall efficiency
The child tries to develop language in both hemispheres, but does not do well in either • This may cause difficulties in speech, reading, writing • Speech may be late in coming and the child usually understands more that he can speak • Once speech develops, it is usually average or close to average, in quality and quantity • Lack of lateralisation skills in children means that there is inadequate communication between the two hemispheres. • When the two sides of the brain cannot communicate, they cannot function in a natural, efficient way.
What should we be looking out for? Child might be seeking/tolerating movement activities such as swinging, running, jumping and does not seem to get dizzy as readily as others Child does not perform well in sports activities May have developed “splinter skills” Falls more frequently that others his age and sometimes make ineffective or no attempts to catch himself or stop himself from falling Feels heavy, like a bag of potatoes, when you try to help him to get into a position, perform an action or to help him get his balance Have difficulty in tasks that require using both hands or both sides of the body, such as cutting with scissors, doing star-jumps, tying shoelaces, riding a bicycle etc.
What should we be looking out for? Have poorly established “handedness” i.e. switches hands for skilled tasks Gets right and left confused Reverses pictures/symbols/letters Avoids crossing the midline of his body by swopping hands or turning whole body to adapt rather than reaching over Have trouble with smoothness of movement and/or rhythm Seems disorganised/lost in space at times
Visual-Motor Development a.k.a. “Copying” • Visual-motor is the first sensory-response integration to develop • Important is the integration of the visual and the motor skills • Children can have well-developed motor and well-developed visual skills but be unable to integrate the two • ”Visual-motor integration is the degree to which visual perception and finger-hand movements are well coordinated.” – Beery • VMI is an outcome of bilateral integration
Letter and number formations • If a child is unable to form numbers or letters correctly, a few factors could play a role: • Motor planning (can the child motor plan when doing self-care tasks such as eating snack/lunch, dressing, tying shoelaces, eating with a knife and fork? Can the child motor plan when doing other fine motor tasks e.g. cutting, sticking and pasting, decorating?) • Muscle development and endurance of the shoulder girdle, arm and hand (are formations consistently poor or do they get progressively worse towards the end of a task?) • Fine motor skills e.g. grasp, fine finger movements, coordination (does the child hold the pencil or other tools correctly? how are the child’s drawing and colouring skills? how do lines connect? can he/she stay on/between lines?) • Visual memory (can the child remember what letters looks like? can the child recognise/identify letters?) • Spatial perception (does the child know right/left on his/her own body? does the child know where right/left is on a page? can the child identify/name similar-looking letters? Can the child copy a simple design correctly and in the same direction?) • Auditory processing (can the child identify the sounds? does he/she know the difference between a b-sound, p-sound and d-sound?)
Reversals • We can not assume that a child will outgrow reversals • It is normal to reverse, but reversals do occur more with dyslexia • Children need a mental age of 5 ½ to 6 ½ to overcome vertical reversals, and 7 ½ for left-right reversals • Reversal co-occurs with poor reading skills • There two types of reversals: • Kinetic reversals are caused by writing or printing in which the child has to move his hand to form a sequence • Static reversals is when there is no movement by the child and he is confused on the proper orientation of the letter or letter sequences in a word as he reads
Basis type of reversal remediationDr. K. Lane • Stage 1: Discrimination stage • Stage 2: Matching to sample tasks • Stage 3: Matching from memory • Stage 4: Letter names • Stage 5: Train in pairs • Stage 6: Train in context • Stage 7: Colour coding • Stage 8: Scanning patterns • Stage 9: Transposing letters within a word and adding or substituting letters • Stage 10: Word reversals
Intervention for reversals • Postural control • Strong intervention on auditory-vestibular-visual triad • Bilateral Integration work • Developmental Optometrist • Ocular-motor home program • Laterality intervention • Reversal program • Remedial therapy
“The resiliency and rapid physical maturation of the infant and young child present an opportunity for developmental neurological change unmatched in any other stage of life. The child’s rapid rate of developmental maturation creates an exceptional opportunity for the experiences of early childhood to shape future capabilities.” (Roley & Blanche & Schaaf, 2001)
References • SI Praxis, Practice and beyond Maude le Roux, 2007 • Sensory Integration and the Child – Understanding hidden sensory challenges A. Jean Ayres, Ph.D., 2005 • Beery VMI – Administration, Scoring and Teaching Manual (5th Edition) Keith E. Beery, Natasha A. Beery, 2006