Understanding and Interpreting Pediatric EKG: A Comprehensive Guide for Clinicians
This resource provides essential insights into reading and interpreting EKGs in pediatric patients. Focused on key components such as P wave, QRS complex, and T wave, it outlines normal heart rates for different age groups. The guide discusses bradycardia and tachycardia, their causes, assessment strategies, and management algorithms. It emphasizes the importance of recognizing signs of poor perfusion and outlines appropriate interventions, including CPR for pulseless rhythms. Clinicians will find detailed information to enhance their skills in pediatric EKG interpretation.

Understanding and Interpreting Pediatric EKG: A Comprehensive Guide for Clinicians
E N D
Presentation Transcript
Reading and Interpreting EKG T Petrillo-Albarano, MD Division of Pediatric Critical Care Children’s Healthcare of Atlanta
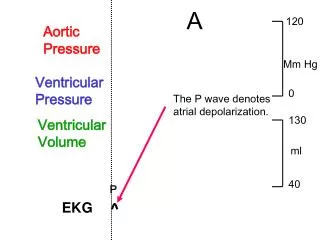
The EKG • P wave • Depolarization atria • QRS • Depolarization ventricle • T wave • Repolarization Ventricle
Normal Rates • O-3 months 85-205 (140) • 3m-2years 100-190 (130) • 2-10years 60-140 (80) • > 10years 60-100 (75)
Identifying Rhythm • Too Slow • bradycardia • Too Fast • tachycardia • Absent • Pulseless arrest
Bradycardia • HR less than 60 • Associated with poor perfusion • Can be caused by many factors • Hypotension, hypoxemia, acidosis, ingestion • In children Hypoxemia is often culprit • Support the airway
Tachy-arrhythmias • ABC • Adequate airway • Respiratory effort • Does the child have a pulse? • No Pulse: CPR; define rhythm • Positive pulse.. Define rhythm • Assess QRS duration
Sinus Tachycardia • Causes? • Hypovolemia • Fever • Anxiety • Pain • Metabolic stressors • drugs
Sinus Tachycardia • P waves present and normal • Variability to rate • Constant PR interval • Infants usually less than 220; children usually less than 180 • Treat the cause
Supra-ventricular Tachycardia • Usual sudden onset • No history to support ST • P waves are often absent ( but can be present) • Abrupt changes • Usually greater than 220 or 180
SVT • Assess Perfusion • Good perfusion: • Call cardiology • Vagal maneuvers • Adenosine • Poor perfusion • Cardioversion • Adenosine • Beta blockers
V Tach with pulse • Most will have underlying congenital heart disease or myocarditis/ cardiomyopathy • Can be related to electrolyte imbalance, toxin, drugs • Cardioversion • Consider Amiodirone
Pulseless Rhythms • VT • V-fib • PEA • Asystole