Urology/Nephrology
Urology/Nephrology. Lecture One – February 21, 2013. Anatomy of the Urinary Tract. Anatomy—Upper Urinary Tract. Kidneys —bean shaped retroperitoneal organs that serve multiple functions in the body 10-13 cm (4-5 in) long 5-7.5 cm (2-3 in) wide. Anatomy—Functions of Kidneys.


Urology/Nephrology
E N D
Presentation Transcript
Urology/Nephrology Lecture One – February 21, 2013
Anatomy—Upper Urinary Tract • Kidneys—bean shaped retroperitoneal organs that serve multiple functions in the body • 10-13 cm (4-5 in) long • 5-7.5 cm (2-3 in) wide
Anatomy—Functions of Kidneys • Waste Excretion – toxins, excess salts, medication, and urea • Hydration Balancing – as fluid intake decreases, kidneys excrete less fluid causing urine to become more concentrated; as fluid intake increases, kidneys excrete more fluid causing urine to become more dilute • Blood Pressure Regulation – kidneys require constant pressure to filter blood; as BP drops kidneys release hormones to increase BP to maintain that pressure
Anatomy—Functions of Kidneys • Red Blood Cell Regulation – decreased O2 leads to release of erythropoietin to stimulate increased RBC production from red marrow • Acid-Base Regulation – Lungs & Kidneys • lungs excrete CO2, at least 12k-13k mmols/day • kidneys excrete fixed acids in blood, 70-100 mmols/day • 2ndextremely important role kidneys play in acid-base balance—reabsorption of filtered bicarbonate, the predominant extracellular buffer against the fixed acids • 2 major activities: Reabsorption of filtered bicarbonate (4k-5k mmol/day) and excretion of the fixed acids (acid anion and associated H+): about 1 mmol/kg/day
Anatomy—Upper Urinary Tract • Ureters– approx. 12 inches long. • 3 layers – fibrous, muscular and mucoid – which are able to contract
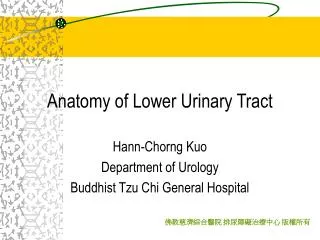
Anatomy—Lower Urinary Tract • Bladder– pelvic organ which acts as a reservoir for urine • Mucoid and muscular layers, surrounded by fascia • Normally holds ~ 400-600 mL • Post-void residual – the amount of urine left in the bladder after the patient has completely voluntarily voided
Anatomy—Lower Urinary Tract • Urethra– connects urinary bladder to genitals for disposal of urine from the body • Female– 1.5-2 inches (4-5 cm) long, exits between clitoris and vagina • Male– 8 inches (20 cm) long, exits at tip of penis and carries semen as well as urine, divided into 4 segments • Pre-prostatic urethra – 0.5-1.5 cm depending on bladder fullness • Prostatic urethra – has prostatic ducts and ejaculatory ducts • Membranous urethra – 1-2 cm portion, narrowest part of urethra, passes through external urethral sphincter • Spongy urethra – runs the length of the penis on its ventral surface, 15-16 cm long, has openings of bulbourethral glands • Length of male urethra and prominent bend makes it more difficult to catheterize a male
Hydrocele • Fluid-filled sac surrounding the testicle resulting in swelling of the scrotum • Congenital, trauma, infection, inflammation, injury
Hydrocele – Signs and Symptoms • Painless, swollen testicle – unilateral or bilateral • May be discomfort from heaviness of a swollen scrotum • May be smaller after first awakening • Exam – swollen scrotum that is not tender • Testicle might not be palpable due to fluid around it • Fluid may be increased / decreased by putting pressure on the abdomen or the scrotum. • Transillumination on exam • US to confirm diagnosis
Hydrocele - Treatment • Benign – usually not dangerous and only treated when they cause discomfort or embarrassment • Hydroceles that do not go away on their own after a few months may need surgery (hydrocelectomyor aspiration)
Varicocele • Enlargement of the veins within the scrotum, along the spermatic cord • Caused by incompetent valves in veins (similar to varicose veins in legs)
Varicocele– Signs and Symptoms • Scrotal Pain • Vary from dull discomfort or heaviness to sharp pain • Increase with sitting, standing or physical exertion • Increase over the course of a day • Relieved by laying flat on his back • Enlarged, twisted veins in the scrotum – twisted growth, classically feels like “bag of worms” on exam • Painless testicular lump, scrotal swelling, or bulge in the scrotum
Varicocele – Treatment • Usually harmless, often does not need treatment • Indicated if pain, testicular atrophy or infertility • Sperm count may improve but fertility does not necessarily improve unless surgery done early in adolescence due to testicular wasting • Scrotal Support • Varicocelectomy • Varicocele embolization
Acute Cystitis • Usually due to coliform bacteria • especially E. coli • gram-positives (enterococci) • Usually ascending infection from urethra • Often seen more in women • Viral cystitis (adenovirus) – may be in children, rare in adults.
Acute Cystitis – Signs/Symptoms • Irritativevoiding symptoms • frequency, urgency, dysuria • Suprapubic discomfort • Gross hematuria • No systemic toxicity
Acute Cystitis • Urinalysis – pyuria, bacteriuria, varying degrees of hematuria, + nitrites • Urine culture is + for offending organism • Imaging – not usually needed for simple, uncomplicated cases • Differential Diagnosis • Women – vulvovaginitis, PID • Men – urethritis, prostatitis • Radiation, chemo, cancer, interstitial cystitis, voiding dysfunction, psychosomatic
Acute Cystitis—Prevention • Women > 3 episodes per year –prophylactic antibiotics • R/O anatomic abnormality • Bactrim (TMP/SMZ) 40/200 mg, nitrofurantoin 100 mg, or cephalexin 250 mg – once daily at bedtime or before intercourse • Catheter-associated UTI • Minimize catheter use and ensure they are removed ASAP • Antimicrobial catheters or external collection devices • Proper insertion techniques • Intermittent instead of continuous caths
Acute Cystitis • Table 23-1, page 914 in Current • Uncomplicated, female patient – short-term antimicrobial therapy such as nitrofurantoin or fluoroquinolone • Men—depends on underlying etiology • Symptomatic – hot sitz baths • Phenazopyridine 200 mg orally 3x/day
Acute Pyelonephritis • Infectious inflammatory disease • Involves renal parenchyma and renal pelvis • Gram-negative bacteria • E. coli, Proteus, Klebsiella, Enterobacter, Pseudomonas • May see Gram-positive – Enterococcus faecalis, Staphylococcus aureus
Signs and Symptoms • Fever • Flank pain • Chills • Shaking • Irritative voiding (urgency, frequency, dysuria) • Nausea • Vomiting • Diarrhea • Fever • Tachycardia • Marked CVA tenderness
Acute Pyelonephritis • CBC – leukocytosis, left shift • Urinalysis – pyuria, bacteruia, hematuria, white cell casts • Urine culture • Blood culture • Imaging
Acute Pyelonephritis • Admit – if severe or complicating factors • Urine and blood cultures • Start empiric antibiotics before sensitivity is back and adjust accordingly • table 23-1, p. 914 • Failure to respond to treatment imaging • Catheter drainage (urinary retention), nephrostomy drainage (ureteral obstruction) • Inpatients – IV antibiotics for 24 hrs after fever resolves • Outpatient oral antibiotics to complete 14-day regimen • Follow up urinalysis / urine culture
Acute Bacterial Prostatitis • Gram negative rods (E. coli, Pseudomonas) less commonly, gram positive (enterococci) • Infection believed to usually to ascend urethra or come from reflux of infected urine to prostatic ducts
Acute Bacterial Prostatitis • Pain – perineal, sacral, suprapubic • Obstructive voiding – varies as prostate swells • Can progress to urinary retention • Fever • Exquisitely tender prostate • Vigorous manipulation of prostate septicemia • Prostatic massage is contraindicated • Labs – CBC – leukocytosis, left shift; UA – pyuria, bacteriuria, hematuria; culture and sensitivity
Acute Bacterial Prostatitis • May need hospitalization if severely ill • IV or oral antibiotics for total of 4-6 weeks of treatment • Table 23-1, p. 914 • Retention catheterization or instrumentation to urethra is contraindicated • Follow-up urine culture and prostatic secretions
Chronic Bacterial Prostatitis • May evolve from ABP, may have no history • Gram negative rods are most common pathogen • Symptoms – some asymptomatic, most have varying degrees of irritative voiding symptoms • Low back pain • Perineal pain • History of UTIs • Exam –often unremarkable • Normal, boggy or indurated prostate all possible
Chronic Bacterial Prostatitis • Urinalysis – normal • Prostatic secretions – increased leukocytes, especially lipid-laden macrophages (>10/hpf) • Culture – prostatic secretions or post-prostatic massage urine specimen • Imaging – not necessary
Chronic Bacterial Prostatitis • Few antibiotics get to therapeutic intraprostatic levels • Trimethoprim/Sulfamethoxazole – associated with the best cure rates • Carbenicillin, erythromycin, cephalexin, fluoroquinolone • Treat for 6-12 weeks • Symptomatic – sitz baths, anti-inflammatory meds • Difficult to cure – control symptoms and recurrent UTIs with suppressive therapy
Nonbacterial Prostatis • Most common form of prostatitis – idiopathic • Chlamydiae, mycoplasma, ureaplasma • Viral • Autoimmune • Diagnosis of exclusion
Nonbacterial Prostatitis • Symptoms – some asymptomatic, most have varying degrees of irritative voiding symptoms • Low back pain • Perineal pain • Identical to chronic prostatitis – but no hx of UTIs • Labs – increased leukocytes on prostatic secretions, but all cultures are negative
Nonbacterial Prostatitis • Trial of antimicrobial therapy (ureaplasma, mycoplasma, chlamydia) • erythromycin 250 mg QID x 14 days • Only continue for 3-6 weeks if clinical improvement • Anti-inflammatory agents • Warm sitz baths • Dietary restrictions only of pt has history of certain dietary triggers
Prostatodynia • Noninflammatory – affects young and middle-aged men • Causes include voiding dysfunction and pelvic floor dysfunction • Prostate is actually normal • Symptoms – chronic prostatitis symptoms • Urinary hesitancy • Interrupted urine flow • Increased anal sphincter tone • Periprostatic tenderness
Prostatodynia • Urinalysis – normal • Prostatic secretions – normal • Urodynamic testing – dysfunctional voiding • Treatment – trial of α-blocker once daily • Sitz baths • Diazepam • Biofeedback techniques
Acute Epididymitis • Sexually Transmitted • Men <40 y/o • Associated with urethritis • Chlamydia trachomatis or Neisseria gonorrhoeae • Non-Sexually Transmitted • Older men • Associated with UTIs and prostatitis • Gram-negative rods
Acute Epididymitis • Symptoms – may follow acute physical strain (heavy lifting), trauma, or sexual activity • Pain in scrotum, may radiate along spermatic cord or to flank • Fever • Scrotal swelling • Tender prostate • urethritis – pain at tip of penis and penile discharge • Cystitis – irritative voiding • Testicle and epididymis may form one swollen, tender mass
Acute Epididymitis • CBC – leukocytosis, left shift • Gram staining of urethral discharge smear • Gram-negative intracellular diplococci (gonorrhea) • White cells without visible organisms (chlamydia) • Urinalysis – pyuria, bacteriuria, hematuria (non-STD)