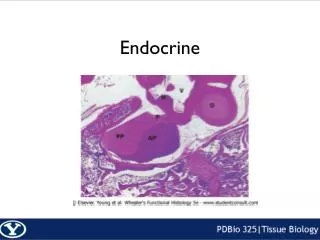
Endocrine Topic
This document outlines essential practices in diabetes care, focusing on early Metformin use, correctional and basal insulin scheduling, and the importance of self-monitoring blood glucose (SMBG). It highlights updated nutritional recommendations and medical nutrition therapy (MNT) for managing diabetes, emphasizing key interventions while referencing the ADA 2007 Standards of Medical Care in Diabetes. Key areas include the role of aspirin, managing diabetic neuropathy, and protocols for hospital and school care settings. These guidelines promote effective diabetes management to improve patient outcomes.

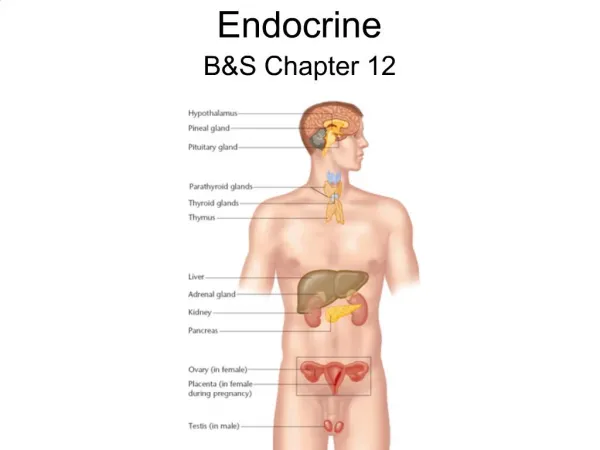
Endocrine Topic
E N D
Presentation Transcript
Endocrine Topic Salyavit Chittmittrapap
Content • 1. Early Metformin Use • 2. Correctional & Basal Schedule Insulin • 3. Aspirin (no new change) • 4. Self monitoring blood glucose (SMBG)
How to get ADA2007pdf • Computer ห้องพักแพทย์In folder “วิชาการแบ่งตามหน่วย” Subfolder Endocrine • Download from Diabetes Care Websitecare.diabetesjournals.org/ • และจะ Upload เอาไว้ที่Website ของภาควิชา
Content of ADA CPR 2007 • Standard of Medical Care in DM 2007 • Diagnosis and Classification of DM • Nutritional Recommendation for DM • Nutritional Intervention for DM What's new
4 3 1 2
Evidence grading (adapted) • A – best ; good RCT !, Meta-analysis, compelling nonexperimental evidence • B – good Cohort study, meta of Cohort, good Case-control study • C – poorly controlled / uncontrolled study observational study, poor RCT, case-series, Conflicting evidence! • E – Expert consensus Not Level of Recommendation
Revised Position statement 1 • Nutrition Recommendations and Interventions for Diabetes: A position statement of the American Diabetes Association • American Diabetes Association Diabetes Care 2007 30: S48-65. • Comprehensive Table3 at pageS58-60
2 Diabetic Peripheral Neuropathy RX
Summary of Revision * * * 3 • Diabetes Care • Comprehensive diabetes evaluation revised • Lowering A1C has been assoc. with a reduction of microvascular & neuropathic complication (A) & possibly macrovascular disease (B) • Medical Nutrition Therapy (MNT) extensively revised
Summary of Revision * * * Nephropathy 3 • Reduction of protein intake to 0.8-1.0 g/kg BW /day in pt. with DM & earlier stage of CKD & to 0.8 g/kg BW /day in the later stage of CKD may improve measure of renal function & is recommended (B) • Celiac disease (child)
Summary of Revision * * * DM care in the hospital 4 • Using correction dose or “supplemental” insulin to correct premeal hyperglycemia in addition to scheduled prandial and basal insulin is recommended (C) • Discontinue ACEI before conception (E) • Diabetes care in the school & day care setting should use a plan (504 plan)by family, school nurse, diabetes health care team
Diabetes Mellitus • Is Chronic illness • Need Continuing medical care • Patient self-management education • Prevent acute complication • Reduce the risk of long-termcomplication
Start with MetforminDon’t wait a second Nathan ET.AL Management of Hyperglycemia in type 2 diabetes consensus statement from ADA and EAstudy of DM. Diabetes Care 29:1963-1972 2006
Target HbA1c <7 % • Keep < 7 % • Reconsider in patient with Short Life expectancy & Terminal illness • Some individual patient benefit from keep HbA1c < 6 % • *with higher Hypoglycemia risk *
After Insulin useDiscontinue Sulfonylurea (or decreased dose)
Thiazolidinedione • After titration of Dose Patient may end up with (Maximal medication) = Intensive insulin with MFM • With or without thiazolidinedione • Actos (15) =42 baht • Avandia (4) =64.5 baht • ADR= fluid retention, Weight gain
Manual adjust Sliding Scale • จริง ๆ แล้วดี เพราะมีการคิดแบบ individual case มองทั้ง insulin maintenance และการตอบสนองต่ออินซูลินครั้งก่อน ๆ • แต่ไม่ดีเพราะแพทย์เจ้าของไข้ไม่ได้อยู่เวรทุกวัน และไม่มีมาตรฐานกลางในการการปรับเปลี่ยนขนาดของอินซูลิน • ไม่ดีเพราะไม่มีการปรับเปลี่ยนขนาดของอินซูลิน ในแต่ละวัน • ทำให้เกิดน้ำตาลสูง / ต่ำ เมื่อ insulin requirement เปลี่ยนแปลง
Correctional dose & Schedule Insulin • เมื่อนำ sliding scale มาปรับปรุงเพิ่มโดยปรับเพิ่ม-ลดในแต่ละวัน ก็ได้เป็น correctional & schedule insulin • มีปริมาณ Basal schedule Insulin คือปริมาณที่คนไข้ที่ระดับน้ำตาลปรกคิต้องการ เป็น maintenance dose • มีการเพิ่มหรือลดปริมาณ insulin ที่ฉีดตามปริมาณน้ำตาลตั้งต้น (DTX) • และสามารถปรับเพิ่มหรือลด scale ตามผลการควบคุมน้ำตาลที่ผ่านมา โดยปรับที่ basal insulin
Correctional dose & Schedule Insulin • Continuous Order • If DTX <60,or >291 please notify • DTX 61-80 decrease insulin 4 u • DTX81-100decrease insulin 2 u • DTX 100-140 no modification • DTX 141-170 increase insulin 2 u • DTX 171-200 increase insulin 4 u • DTX 201-230 increase insulin 6 u • DTX 231-260 increase insulin 8 u • DTX 261-290 increase insulin 10 u • One day Order • RI 10 – 10 – 10 sc ac • Monotard 10 u sc hs.
Example . DM male 55yrs on oral feeding • Previously need total insulin 40 u /day • Start with 10 u basal insulin • DTX morning 145 RI 12 u • DTX noon 70 RI 6 u • DTX evening110 RI10 u • DTX hs90 Monotard 8 u • Continuous Order • DTX 61-80 decrease insulin 4 u • DTX81-100decrease insulin 2 u • DTX 100-140 no modification • DTX 141-170 increase insulin 2 u • DTX 171-200 increase insulin 4 u • DTX 201-230 increase insulin 6 u • One day Order • RI 10 – 10 – 10 sc ac • Monotard 10 u sc hs. • TOTAL TODAY 36
Example . DM male 55yrs on oral feeding • Previously need total insulin 40 u /day • Start with 10 u basal insulin • DTX morning 145 RI 12 u • DTX noon 190 RI 14 u • DTX evening180 RI14 u • DTX hs220 Monotard 16 u Correctional Insulin 16 u thenIncrease Basal inuslin • Continuous Order • DTX 61-80 decrease insulin 4 u • DTX81-100decrease insulin 2 u • DTX 100-140 no modification • DTX 141-170 increase insulin 2 u • DTX 171-200 increase insulin 4 u • DTX 201-230 increase insulin 6 u • One day Order • RI 10 – 10 – 10 sc ac • Monotard 10 u sc hs. • TOTAL TODAY 56
Benefit • Hypoglycemic Symptom = Hypoglycemia ? • Better Glycemic control • Cost ; ค่าเครื่อง (1800) • ค่าแถบตรวจน้ำตาล (9) • สำคัญกว่าคือใช้ให้ได้ประโยชน์ DM type 1 GDM
Thailand situation; Beware ! • Increased RISK OF BLEEDING • NSAID abuse • Regular NSAID uses • Untreated Peptic Ulcer • Uninvestigated Dyspepsia • Undetected (&Untreated H.Pylori)
Landmark Paper for starting metformin immediately after Diagnosis of DM
OGTT is bettertest with much complicated steps , used limitedly eg. After IFG
GDM • Develop DM after Pregnancy = overt DM • Different number from harrison Harrison target Fasting <105 Post Prandial <120
High Risk modest wt. loss, regular physical activity. Esp with IGT*** (A) • For IFG same (E) • Follow up counseling appears to be important for success (B) • Monitor DM in pre-DM q 1-2 years (E) • No Medication !!!
Reduce Risk & Slow progression of DN by Blood Pressure & Glucose control (A) • Screen Microalbuminuria annually • - type 1 ; 5yrs or more after DX • - type 2 ; at DX • - during Pregnancy (E) • Screen serum Cr annually(E)
ACEI & ARB • No Winner !!!
If cannot use ACEI & ARB ; Betablockers, Diuretics, Non-DCCBs is considered(E) New Check K
Reduce Risk & Slow progression of DR by Blood Pressure & Glucose control (A) • ASA does not prevent DR nor increase the risks of hemorrhage (A) • Screen by Opthalmologist or Optometrist • Screen annually ; start at • - type 1 ; 3-5yrs or more after DX • - type 2 ; at DX (B) Pregnant = risk progress DR Check DR at preg, along and 1yr post partum
A. Cardiovascular Diseases • 1. BP control • 2. Dyslipidemia • 3. ASA (detail=above) • 4. Smoking cessation • 5. CHD screening & treatment
=Plasma glucose <70 mg/dl • Repeat after RX at 15 min (B) • Glucagon use (E)
K. Immunization • Annual Influenza virus (C) • One (lastlong) Pneumococcal Vaccine • Repeat if >65 yrs with recent vaccine >5 yrs • Repeat if Nephrotic Syndrome, CKD, immunocompromised state
Take Home Message • You should start Metformin after dx DM • Correctional dose & Schedule Insulin • DM+DN ; diabetic diet, Protein 0.8-1.0 g/kgBW/d(0.8 for Late CKD), low fat • Advice symptom of DKA-HHS and also Stroke & MI • ASA gr.I 2*1 with discussion of benefit & risk