Download
1 / 1
10 likes | 168 Vues
Comparison of Medicare Claims vs. Physician Adjudication for Identifying Cardiovascular Outcomes in the Women’s Health Initiative. Dale R. Burwen 1 , Garnet Anderson 2 , Dominic Cirillo 3 , Mark Hlatky 4 , Kamakshi Lakshminarayan 5 , Joseph Larson 2 , Marian Limacher 6 ,

E N D
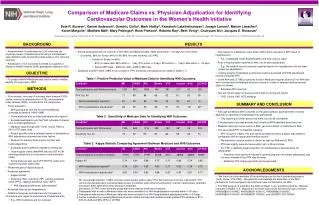
Comparison of Medicare Claims vs. Physician Adjudication for Identifying Cardiovascular Outcomes in the Women’s Health Initiative Dale R. Burwen1, Garnet Anderson2, Dominic Cirillo3, Mark Hlatky4, Kamakshi Lakshminarayan5, Joseph Larson2, Marian Limacher6, Karen Margolis7, Matthew Mell4, Mary Pettinger2, Ross Prentice2, Roberta Ray2, Beth Virnig5, Chunyuan Wu2, Jacques E. Rossouw1 1National Heart, Lung, and Blood Institute, Bethesda, MD; 2Fred Hutchinson Cancer Research Center, Seattle, WA; 3University of Iowa, Iowa City, IA; 4Stanford University, Stanford, CA; 5University of Minnesota, Minneapolis, MN; 6University of Florida, Gainesville, FL; 7HealthPartners, Minneapolis, MN RESULTS BACKGROUND • Ascertainment of cardiovascular (CV) outcomes via physician review of medical records using a standardized case definition aims to maximize data quality, but is resource intensive. • Adjudication of CV outcomes is limited to a quarter of Women’s Health Initiative (WHI) participants starting in 2010. • To assess whether Medicare data can be used to reliably identify CV outcomes in WHI. • Four projects, focusing on coronary heart disease (CHD), stroke, venous thromboembolism (VTE), and peripheral artery disease (PAD), contributed to this comparison. • Study population • WHI participants with fee-for-service Medicare coverage at baseline (1993-1998) • Some analyses also included participants who aged in • Excluded participants who had WHI outcome of interest prior to entering Medicare • Medicare data through 2007 (CHD, stroke, PAD) or 2010 (VTE) were used • Project specific cohorts selected based on availability of WHI adjudicated outcomes and other factors • Divided into training (data shown) and test sets • Coding algorithms • Evaluated and modified as needed in training set • Used hospital claims (MedPAR file) and ICD-9-CM discharge diagnoses (in any position) and procedure codes • Some analyses also used CPT/HCPCS codes from Carrier/Outpatient claims files • Performed person-based analysis • Assessed agreement • Kappa statistic • Sensitivity (SN), specificity (SP), positive predictive value (PPV), negative predictive value (NPV) • WHI diagnosis defined as “gold standard” • Assessed reasons for disagreement • Additional analyses excluded records that were not informative with regard to performance of Medicare data • E.g., WHI medical record not received • Among participants with an outcome in both WHI and Medicare data, dates were within +/-30 days for most events • Examples: 96% for Stroke; 94% for MI; 85% for lower extremity (LE) PAD • Details for Stroke (n=505): • 83% on same date; 88% within +/- 1 day; 91% within +/-3 days; 95% within +/- 7 days; 96% within +/- 30 days • Range (WHI date – Medicare date) -4269 to 682 days • Specificity and NPV were >98% for all conditions; PPV, sensitivity, and kappa are provided in Tables 1-3 • Key reason for a Medicare event without WHI match was lack of WHI report of hospitalization • E.g., Inadequate recall; disability/death and lack of proxy report • Even if hospitalization reported to WHI, not all were adjudicated • E.g., No medical records received; reported reason for hospitalization did not meet criteria for adjudication • Limiting analysis to Medicare events that could be evaluated with WHI adjudicated records increased PPV • Some AAA and LE PAD procedures found in Medicare hospital claims but not WHI data were corroborated by Medicare physician claims or review of selected medical records (data not shown) • Estimated PPV was high • Test set results (data not shown) were similar to training set results • CHD, Stroke, PAD (VTE pending) • Although we defined WHI outcomes as the gold standard, ascertainment of events depends on reporting of hospitalization by participants • This reporting is similar across trial arms, but can be incomplete • The adjudication process ensures that virtually all WHI identified events are true • Medicare data miss some events in WHI, yet record others not identified in WHI • The associated PPV is imperfect, however • PPV is high for CABG, PCI and carotid procedures (when analysis was limited to participants with an adjudicated medical record) • We estimate it may be similar or almost as high for AAA and LE PAD • PPV was slightly lower but reasonably high for MI and stroke • For VTE, a relatively larger proportion of hospitalizations reported were not adjudicated • Therefore more caution is needed in generalizing from the subset adjudicated, and the best estimate of the PPV may be lower • Additional VTE coding algorithms are being tested • We thank the other members of the working groups for the 4 contributing projects (CHD, stroke, VTE, PAD). We gratefully acknowledge the dedication of the WHI participants, and investigators and staff who have contributed to the WHI. • The WHI program is funded by the National Heart, Lung, and Blood Institute, National Institutes of Health, U.S. Department of Health and Human Services through contracts HHSN268201100046C, HHSN268201100001C, HHSN268201100002C, HHSN268201100003C, HHSN268201100004C, and HHSN271201100004C. OBJECTIVE Table 1. Positive Predictive Value of Medicare Data for Identifying WHI Outcomes. METHODS SUMMARY AND CONCLUSION Table 2. Sensitivity of Medicare Data for Identifying WHI Outcomes. Table 3. Kappa Statistic Comparing Agreement Between Medicare and WHI Outcomes. ACKNOWLEDGMENTS * MI, myocardial infarction; CABG, coronary artery bypass graft surgery; PCI, percutaneous coronary intervention; VTE, venous thromboembolism (including deep venous thrombosis and pulmonary embolism); Carotid, carotid artery treatment procedure; AAA, abdominal aortic aneurysm treatment procedure; LE PAD, lower extremity peripheral artery disease treatment procedure † Participants with events in Medicare data only were excluded if no WHI hospitalization recorded within +/-30 days ‡ Participants with events in Medicare data only were excluded if no WHI hospitalization adjudicated within +/-30 days §Further evaluation by reviewing Medicare physician claims and selected medical records yielded PPV estimate of 91%- 94% for AAA and 92%-95% for LE PAD