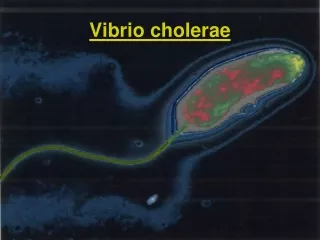
Vibrio and Pseudomonas
A 57-year old man was hospitalized in New York with a 2-day history of severe, watery diarrhea. The illness had begun 1 day after his return from Ecuador. The patient was dehydrated and suffering from an electrolyte imbalance (acidosis, hypokalimea).

Vibrio and Pseudomonas
E N D
Presentation Transcript
A 57-year old man was hospitalized in New York with a 2-day history of severe, watery diarrhea. The illness had begun 1 day after his return from Ecuador. The patient was dehydrated and suffering from an electrolyte imbalance (acidosis, hypokalimea). The patient made an uneventful recovery after fluid and electrolyte replacement was instituted to compensate for the losses resulting from the watery diarrhea. Stool cultures were positive for ….
Vibrio and Pseudomonas Vibrio cholerae Vibrio parahaemolyticus Vibrio vulnificus Pseudomonas aeruginosa
Vibrio V. choleraeV. parahaemolyticus Gram-negative Comma-shaped Facultatively anaerobic Can grow in the absence of salt Single polar flagellum
Vibrio The O polysaccharide of the LPS is used to subdivide Vibrio species into serogroups: V. choleraeO1 and O139 > classic cholera V. cholerae O1 serogroup is divided further into biotypes "el tor” classical (cholerae)
Protective gear against cholera in early 19th century Germany
Vibrio Pathogenesis Cholera toxin ("choleragen”) encoded by bacteriophage CTXø A-B structure 5 B subunits bind to gangliosides on mucosal cells (ctxB gene) A subunit ADP-ribosylates the Gs protein (ctxA gene) Activates adenylate cyclase
Vibrio Pathogenesis Accumulation of cAMP Secretion of chloride, bicarbonate and water into the intestinal lumen Fluid loss in severely infected patients 1 liter of fluid per hour
Pathogenesis Toxin co-regulated pilus (tcp gene) Adherence to intestinal mucosal cells Binding site for bacteriophage CTXø Colonization factor (cep gene) Adhesin molecules mediate adhesion to the mucosal cell surface
Pathogenesis Accessory cholera entereotoxin (ace gene) Increased fluid secretion Zonula occludens toxin (zot gene) Loosens the tight junctions of the small intestine mucosa Hemagglutinin-protease (hap gene) Mucinase: Dissolves the protective glycoprotein coating over intestinal cells
Attachment of V. cholerae to M cells in human ileal mucosa Attachment of V. cholerae to the brush border
Pathogenesis Vibrio parahaemolyticus Thermostable direct hemolysin “Kanagawa hemolysin” Induces chloride ion secretion by increasing intracellular calcium Causes ß-hemolysis on agar media with human blood (Kanagawa-positive)
Transmission Vibrio Grow in estuarine and marine environments, particularly those with chitinous shellfish Transmitted by contaminated water and food Seven major pandemics since 1817
Transmission V. parahaemolyticus and V. vulnificus Via improperly cooked seafood (oysters!) and exposure to contaminated seawater V. parahaemolyticus Most common cause of bacterial gastroenteritis in Japan and Southeast Asia Most common Vibrio species responsible for gastroenteritis in the US
Spread of O1 El Tor starting in 1961 in the Philippines From Todar’s Online Textbook of Bacteriology
Spread of pandemic V. cholerae O1 El Tor in the Americas 1991-1994
Clinical syndromes Vibrio cholerae Watery diarrhea and vomiting Rice-water stools Fluid loss >dehydration > metabolic acidosis (bicarbonate loss) > hypovolemic shock (abnormally decreased plasma volume) >cardiac arrhythmia >renal shock
Science sleeps on a New York dock as Cholera floats across the ocean from Europe
Clinical syndromes Vibrio parahaemolyticus Watery diarrhea Headache Abdominal cramps Nausea Vomiting Low grade fever May persist for 72 h or more
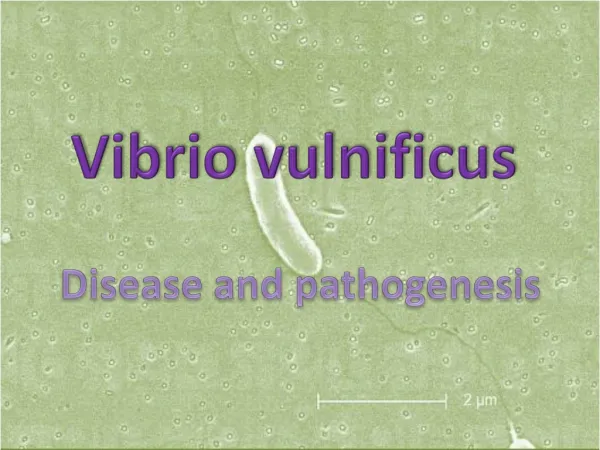
Clinical syndromes Vibrio vulnificus Rapidly progressive wound infections after exposure to contaminated seawater Initial swelling, erythema, pain Development of vesicles, tissue necrosis Septicemia after exposure to contaminated raw oysters Mortality can be as high as 50% if antimicrobial treatment is not started promptly Infections most severe in patients with hepatic disease, hematopoietic disease, and those receiving immunosuppressive drugs
Treatment and control Vibrio cholerae Fluid and electrolytes before hypovolemic shock Doxycyline, tetracycline: reduce exotoxin production Furazolidone for pregnant women Trimethoprim-sulfamethoxazole for children Improved sanitation: sewage; water purification Killed cholera vaccine: short lived protection
Treatment and control Vibrio parahaemolyticus Usually self-limiting Fluid and electrolyte therapy Antibiotics Vibrio vulnificus Immediate treatment with Minocyline, and a fluoroquinolone or cefotaxime
Pseudomonas aeruginosa Aerobic, Gram-negative bacilli In soil, decaying organic matter, vegetation and water In hospitals: food, cut flowers, sinks, toilets, floor mops, equipment for respiratory therapy and dialysis In hexachlorophene-containing soap solutions and disinfectant solutions
Pseudomonas aeruginosa Pathogenesis Adhesins Bacterial neuraminidase Polysaccharide capsule Endotoxin Exotoxin A Blocks protein synthesis ADP-ribosyltransferase Tissue damage in burn wound, chronic pulmonary and ocular infections
Pathogenesis Exoenzymes S and T ADP-ribosyltransferase Interferes with phagocytic killing Cause epithelial cell damage, via actin rearrangement Elastases > lung parenchymal damage,hemorrhagic lesions (ecthyma gangrenosum) Degrade complement, inhibit PMN chemotaxis Phospholipase C
Pathogenesis Pyocyanin Impairs ciliary function Stimulates IL-8 release (neutrophil migration) Mediates tissue damageviaproduction of superoxide and hydrogen peroxide (in the presence of pyochelin, a siderophore) Antibiotic resistance Mutation of porin proteins b-lactamase production
Pseudomonas aeruginosa Transmission Ubiquitous opportunistic pathogen Persistent carriage common in hospitalized patients
Pseudomonas aeruginosa Transmission Risk factors Prior treatment with broad-spectrum antibiotics Respiratory therapy Prolonged hospitalization Compromised immune function Exposure to contaminated water Diabetes Old age iv drug use
Pseudomonas aeruginosa Clinical syndromes Most commmon infections Urinary tract infections Pneumonia (in Cystic Fibrosis) Wound infections (burns)
Pseudomonas aeruginosa Clinical syndromes Pulmonary infections From benign tracheobronchitis to severe necrotizing bronchopneumonia Cystic fibrosis> involvement of pulmonary parenchyma Cystic fibrosis>P. aeruginosa initiates a rapid mutation rate
Pseudomonas aeruginosa Clinical syndromes Primary skin infections Mostly in burn wounds Localized vascular damage Tissue necrosis Bacteremia
Ecthyma gangrenosum in a child with Pseudomonas septicemia associated with immunodeficiency Due to degradation of elastin by bacterial elastase
Pseudomonas aeruginosa Clinical syndromes Ear infections External otitis Most frequently caused by P. aeruginosaSwimming is a risk factor Malignant external otitis (elderly and diabetics) Damage to nerves and bone Chronic otitis media
Pseudomonas aeruginosa Clinical syndromes Eye infections Bacteremia Mostly in patients with neutropenia, diabetes, extensive burns and hematological malignancies Mortality rate > 50% Endocarditis Mostly in iv drug users
Pseudomonas aeruginosa Treatment and control Resistant to most antibioticsResistance can develop during therapy ß-lactamases, plasmid-mediated transfer Combination of aminoglycosides (poor activity in the acidic environment of an abscess) and ß-lactam antibiotics (e.g., ticarcillin or piperacillin) Hyperimmune serum Granulocyte transfusions
Pseudomonas aeruginosa Treatment and control Avoid contamination of sterile equipment Avoid contamination of patients by medical personnel Remove indwelling catheters promptly Take special care of burned skin