Download
1 / 34
440 likes | 1.63k Vues
Dr Cheng Wing Ho Stephen ICU, Pamela Youde Nethersole Eastern Hospital Friday Meeting Jan 21 , 2011. Carbapenem -Resistant Enterobacteriaceae (CRE). Overview. What is CRE? Mechanism of resistance International cases 3 recent cases in Hong Kong Possible treatment options

E N D
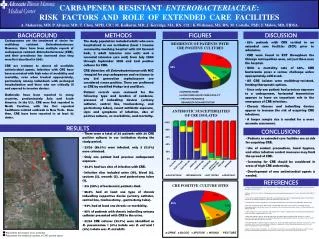
Dr Cheng Wing Ho Stephen ICU, Pamela Youde Nethersole Eastern Hospital Friday Meeting Jan 21, 2011 Carbapenem-Resistant Enterobacteriaceae (CRE)
Overview • What is CRE? • Mechanism of resistance • International cases • 3 recent cases in Hong Kong • Possible treatment options • HA / CDC guidelines on infection control
Background Enterobacteriaceae • Gram -ve bacilli • Facultative anaerobes • Gut flora, or found in soil / water • Common causative agents of UTI, pneumonia Examples: • E. coli, Klebsiella, Salmonella, Shigella, Proteus
Background • Treatment options • Penicillin (e.g. ampicillin, amoxicillin, piperacillin) • Cephalosporin (e.g. cefuroxime, ceftriaxone) • (combined with β-lactamase inhibitor) Augmentin, Tazocin, Sulperazone • Carbapenem (e.g. imipenem, ertepenem, meropenem) • Quinolone (eg. ciprofloxacin, levofloxacin) • Extended-spectrum-β-lactamase strains • only sensitive to carbapenem group and limited penicillin/cephalosporin coupled with β-lactamase inhibitors
What is CRE? • Enterobacteriaceae strains resistant to carbapenem have emerged in the past decade • Wide-spread outbreaks have been reported in recent years • No reliable treatment options • Huge reservoir of carriers in healthy population • Easy species-to-species spread • Potential devastating health consequences
Mechanism of resistance • Carbapenemase • b-lactamase • hydrolyzing agent • 4 classes (A-D): serine vs zinc • produced by ‘Superbugs’ • Klebsiella Pneumoniae Carbapenemase (KPC) • Verona integron-encoded metallo-β-lactamase (VIM) • Oxallinase group β-lactamase (OXA) • SME, IMI, NMC and CcrA (little clinical significance)
Carbapenemase • Klebsiella Pneumoniae Carbapenemase (KPC) • first detected in 1996 • most commonly expressed in K. pneumonia • also reported in Citrobacter, Enterobacter , E. coli, Salmonella, Serratia • class A b-lactamase • causes resistance to all b-lactams including extended-spectrum cephalosporins and carbapenems
Carbapenemase • KlebsiellaPneumoniaeCarbapenemase (KPC) • encoding gene blaKPC carried on plasmids • reported to be found on plasmids with • normal spectrum b-lactamases • extended spectrum b-lactamases • aminoglycoside resistance • fluoroquinolone resistance leads to extensive-drug resistance (XDR) • virulence factors on plasmids • easy transmission of self-reproducing plasmid between species
Statistical data on KPC • European Antimicrobial Resistance Surveillance System (EARSS) • CRKP in 0.3% of blood isolates prior to 2006 • following an outbreak in 2006 in Israel 11% in 2006, 22% in 2007 • mortality associated with CRKP isolation up to 44% • standardized morality rate ~8 deaths per 100,000 • compared to 6 deaths per 100,000 of MRSA (2005) Predictors of CRKP acquisition among hospitalized adults and effect of acquisition on mortality. Antimicrob Agents Chemother. 2008;52(3):1028-1033
A new carbapenemase • New Delhi metallo-b-lactamase (NDM-1) • class B b-lactamase • plasmid carrying encoding gene blaNDM • first detected in 2009 from an isolate of K. pneumoniae • Swedish patient with antibiotic-resistant infection acquired and unsuccessfully treated in New Delhi, India • novel gene identified in Sweden
A new carbapenemase 14 out of 24 patients come from ICU “New Delhi Metallo-β lactamase (NDM-1) in Enterobacteriaceae: Treatment options with Carbapenems Compromised”. Journal of Association of Physicians of India 58: 147–150, March 2010 • New Delhi metallo-b-lactamase (NDM-1) • over a 3-month period in Mumbai, India, 24 cases of carbapenam resistant isolates were identified • 22 carry the NDM-1 gene • K. pneumoniae (10) • E. coli (9) • 14 samples from ICU • Carbapenem-resistance 0% 8% in 3 years
Latest situation • Emergence of a new antibiotic resistance mechanism in India, Pakistan, and the UK: a molecular, biological, and epidemiological study Lancet Infect Dis. 2010 September ; 10(9): 597–602 • UK (37) - all had travelled to India/Pakistan • Chennai (44), Haryana (26) • other sites in India and Pakistan (73) • K. pneumoniae (111) • E. coli (36) • Globally, estimated 250 identified isolates so far http://www.ndm1bacteria.com
Global spread of NDM-1 • May 2010, first E.coli isolate in UK • Indian man received dialysis in India 18 months ago • June 2010, 3 Enterobacteriaciae strands in US • all received medical procedures in Indian hospitals previously • July 2010, 3 isolates of Acinetobacterbaumannii in New Delhi, ICU • August 2010, first identified case in Ontario, Canada • September 2010, first case in Tokyo, Japan
First death case • August 2010 • Belgian man • road-traffic-accident in Pakistan • hospitalized for major leg injury • infected with an isolate of NDM-1 • succumbed despite use of Colistin
CLSI guidelines for Laboratory workup for CRE • Enterobacteriaceae resistant or moderately resistant to Carbapenem PCR test for carbapenemase gene • Isolates that are susceptible but with increased minimal inhibitory concentrations (MIC) Modified Hodge Test • If positive Modified Hodge Test • proceed to PCR test for gene identity • manage as CRE test sample -ve control +ve control Clinical and Laboratory Standards Institute. 2009 performance standards for antimicrobial susceptibility testing. 2009.
In Hong Kong • Incidence of CRE in 2009 is about 0.05% • 8 isolates carrying the metallo-b-lactamases (IMP type) • E. coli, Klebsiella spp. and Citrobacter freundii • Mostly colonizing flora • No cases of KPC isolates detected so far • 2 cases of recently identified New Delhi metallo-b-lactamase isolate An overview of surveillance of antimicrobialresistance by CHP in Hong Kong Communicable Diseases Watch 2010; Volume 7, Number 17. Aug 2010
The 2 NDM-1 cases in Hong Kong • Case 1 (October 2010) • 66 year old Indian man • out-patient • followed up for hypertension, diabetes • treated for UTI that responded to ciprofloxacin • NDM-1 carrying E. coli detected in urine culture • history of spending 3 weeks in India in March 2010 • no history of hospitilization in India • full recovery
The 2 NDM-1 cases in Hong Kong • Case 2 (December 2010) • 54 year old Indian lady • treated for subdural hematoma in India from May to August 2010 • attended and admitted to PMH on Dec 17 for respiratory distress • NDM-1 carrying E. coli detected in rectal swab • likely colonization due as no evidence of infection
Our recent CRE case in PYNEH • ICU in-patient in D10 (January 2010) • 83 year old Chinese man • recent hospitilization in the Philippines • biliarypapillomatosis • admitted for robotic assisted laparoscopic L hepatectomy, complicated with leakage • CRE was cultured from bile • only sensitive to Gentamicin (treated with Tazocin) • PCR test positive for VIM gene (class B) • patient discharged home • case reported and contact tracing underway
Polymyxin • Cyclic peptide with hydrophobic tail • Produced by Bacillus polymyxa • Selectively targets Gram-ve bacteria by disrupting both outer and inner membranes • Polymyxin B • Colistin (polymyxin E) • Only effectively via parenteral route • No guidelines for standard / optimum / max dose • Nephrotoxic and neurotoxic • Shown to be useful against MRAB, Pseudomonas
Tigecycline • Glycylcyline, derivative of tetracycline • Protein synthesis inhibitor • Targets Gram+ve, Gram-ve bacteria, anaerobes • No activity against Pseudomonas, Proteus • Licensed for treating skin infection, intra-abdominal infections • 100mg IV stat followed by 50mg Q8H • Side effects profile similar to tetracycline: GI upset, photosensitivity, teeth discoloration, fetal damage
Other possible drugs • NXL104 • novel non-β-lactam β-lactamase inhibitor • use in combination with Ceftazidime • GSK 299423 (GlaxoSmithKline 299423) • inhibits the enzyme topoisomerase • effective in clearing NDM-1 • ACHN-490 and other Aminoglycosides • no activity against the NDM-1 isolates
HA guidelines on CRE • From data of other countries, KPC associated infections are mostly systemic infections • NDM-1 associated infections are usually UTI, pneumonia, and blood stream infection • Risk factors: • prolonged hospitalization • ICU stay • invasive devices • immunosuppression • prior use of multiple antibiotics Infection Control Guideline on Carbapenem Resistant Enterobacteriaceae (CRE), Hospital Authority, 1 Dec 2010
Infection control strategies 1) Prudent antibiotic use • Antibiotic Stewardship Program (ASP) should be in place to give advice on and monitor the appropriate use of antimicrobials in patient care 2) Early detection of CRE • Active surveillance culture (ASC) - rectal swab/stool culture for patients hospitalized outside Hong Kong in the last 6 months • Screen carriage for same cubicle in-patients (>=2 days) of PCR +ve CRE, inform Infection Control Branch if discharged to elderly home, institutions Infection Control Guideline on Carbapenem Resistant Enterobacteriaceae (CRE), Hospital Authority, 1 Dec 2010
Infection control strategies 3) Review of microbiology record of previous 6-12 months • detect unrecognized cases • if cases identified • point prevalence survey (a single round of active surveillance cultures) in high risk units Example: • ICU • units where the identified case previously occupied • units exposed to broad-spectrum antimicrobials 4) Laboratory protocols for detecting CRE Guidance for Control of Infections with Carbapenem-Resistant or Carbapenemase-Producing Enterobacteriaceae in Acute Care Facilities, March 2009
When CRE is confirmed... 1) Infection control measures: • Single room isolation • discontinue when infected site cleared or eradication of carriage in gut (culture negative for at least 2 consecutive stool/ rectal swabs collected at 48 hours interval) • Contact precautions • Hand hygiene • Dedicated equipments • Enhance / terminal environmental cleansing • Minimize patient transfer • Advice to visitors Infection Control Guideline on Carbapenem Resistant Enterobacteriaceae (CRE), Hospital Authority, 1 Dec 2010
When CRE is confirmed... 2) Alert and reporting: • Inform the Chief Infection Control Officer’s Office (CICO Office) of any patient with PCR +ve CRE or when an outbreak of CRE is suspected • MHT positive cases should label in the CMS alert ‘Carbapenemase producing Enterobacteriaceae detected’ • Revise CMS alert to ‘CRE PCR +ve’ if PCR tested positive • The alert should be removed when the patient has been eradicated of CRE • When CRE PCR +ve patient is re-admitted, infection control precautions should taken and ICT informed Infection Control Guideline on Carbapenem Resistant Enterobacteriaceae (CRE), Hospital Authority, 1 Dec 2010
When CRE is confirmed... 3) Transfer / discharge issues • ICT involved in all inter-hospital or intra-hospital transfer of CRE +ve patient • Discharge to institutions / elderly home • should have 2 consecutive negative screening culture at 48 hours interval. ICB must be informed • asymptomatic prolonged CRE carriage (e.g. >=8 weeks) must be risk assessed jointly by the hospital ICT, CICO and ICB • Patients discharged home should be given education pamphlet on infection control precautions • Patients with CRE +ve confirmed after discharge should be contacted for information and education on infection control precautions Infection Control Guideline on Carbapenem Resistant Enterobacteriaceae (CRE), Hospital Authority, 1 Dec 2010
Bring home message • Carbapenem-Resistant Enterobacteriaceae is an emerging threat to hospitalized patients • Global spread • High mortality • Treatment options are limited • Active surveillance should be performed for high risk patients with overseas hospitalization in past 6 months • Contact tracing / screening for confirmed cases • Importance of infection control measures • High vigilence in critically ill ICU patients
Thank you! The End