Botulism
Botulism. Dr/ Mona M. Awny Assistant lecturer of forensic medicine & clinical toxicology. Food poisoning. Most common bacterial food-borne pathogens: Clostridium botulinum Clostridium perfringens Escherichia coli Staphylococcus aureus Bacillus cereus Vibrio cholera.

Botulism
E N D
Presentation Transcript
Botulism Dr/ Mona M. Awny Assistant lecturer of forensic medicine & clinical toxicology
Food poisoning Most common bacterial food-borne pathogens: • Clostridium botulinum • Clostridium perfringens • Escherichia coli • Staphylococcus aureus • Bacillus cereus • Vibrio cholera
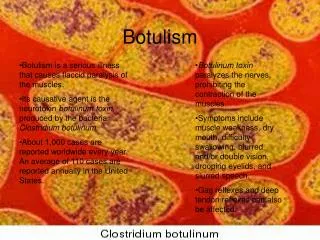
Clostridium botulinum? • Gram +ve anaerobic bacillus that release neurotoxin “Botulin”.
Clostridium botulinum: • Toxin types: • A / B / C alpha / C beta • D / E / F / G • Physical properties: - Spores withstand 100 c for hours. - Toxins are heat-labile and destroyed by boiling for 10 min. or heating at 80 c for 30 min.
Food sources Mainly not exposed to heat: Salted fish “Fesikh” Honey Uncooked cold meat “Beef” Home canned food
BotulismFatal condition caused by ingestion of improperly preserved or canned food Types of Botulism • Food related botulism: Classic botulism and Infant botulism • Wound botulism
Dissemination of toxins • Toxins are distributed to target sites via hematogenous dissemination
Mechanism of action “Neurotoxicity” • Toxins act on the presynaptic part of neuromuscular junctions leading to decreasing the amount of ACH release
Clinical presentation • Symptoms & signs develop within 12 – 36 hrs after ingestion • Severity of disease depends on type of toxin (type A gives most severe picture) • GIT symptoms • Anticholinergic symptoms • Neurological symptoms
Initial vague & GIT symptoms: • Malaise, weakness, dizziness, diplopia & blurred vision • Nausea, vomiting, diarrhea or constipation
Dry mucous membranes • Markedly dilated pupils & blurred vision • Urinary retention (palpable urinary bladder) • Absent bowel sounds & abdominal distention • Nohyperthermia or tachycardia
Neurological manifestations: • Cranial nerve palsy • Bilateral symmetrical descending flaccid paralysis of: 1. Bulbar musculature 2. Limbs 3. Resp. muscles & diaphragm • No sensory loss • Normal mental status
Motor cortex Bulb/brainstem Bulbar musculature Bulbar musculature • Eye movement • M. of facial expression • Speaking & swallowing
No sensory loss • Normal mental status • Death from respiratory failure
Investigations • General tests: • ECG • Abdominal U/S • CSF • Pulmonary function tests • ABG
Investigations • Toxin-specific tests: • C. botulinum toxin or sporesin serum, stool, gastric contents or wound specimens • Electromyography (EMG): • Shows a defect in transmission at the neuromuscular junction
Differential diagnosis • Guillian-Barre syndrome: • Ascending paralysis, ↑CSF protein, normal EMG • Cerebrovascular stroke: • Asymmetric • Poliomyelitis: • Fever & meningeal signs • Anticholinergic poisoning: • Fever & altered mental status
Management • General: • ABC’s (early elective tracheostomy & mechanical ventilation) • Emesis & gastric lavage • Nasogastric suction (ileus) • Foley catheterization (urine retention)
Management • Toxin-specific measures: • Trivalent ABE antiserum • Sensitivity test • Dose:1 vial IM & 1 vial IV • A dose/ 4hrs if serum toxin persists
Follow-up & disposition • Admission to ICU • Monitoring of vital capacity & vital signs • Prolonged hospitalization • Slow recovery • Rehabilitation program • Complete recovery of paralysis takes up to 6 months
Wound botulism • Soil • Symptoms • Wound swab • Antitoxin, debridement, high-dose IV penicillin