Download
1 / 24
240 likes | 330 Vues
Learn about foodborne botulism, its clinical features, symptoms, treatment, and public health implications. Understand NYC Dept. of Health roles and challenges in managing botulism outbreaks.

E N D
FOODBORNE BOTULISM NYC Dept. of Health and Mental Hygiene Office of Emergency Preparedness and Response
OBJECTIVES • Review DOHMH roles and responsibilities during a foodborne botulism incident • Discuss ways to address potential planning gaps and incident-related challenges
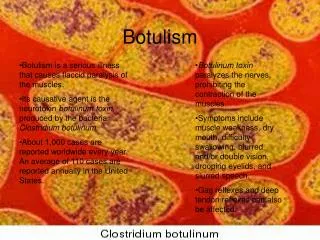
GENERAL • Botulism is a paralytic illness caused by a neurotoxin that is produced by an anaerobic bacterium, Clostridium botulinum • Toxin absorbed in the digestive tract binds irreversibly to structures in voluntary/involuntary motor nerves, inhibiting secretion of a neurotransmitter and transmission of nerve impulses • This leads to weakness or paralysis of affected motor nerves, including those governing respiration • Botulinum toxin is heat-sensitive and is inactivated in food when the temperature is kept above boiling for 10 minutes • Sensory nerves are unaffected. • Human botulism is caused by toxin types A, B, E and F. • Waterborne botulism has never been documented • Successful contamination of large water supplies is unlikely because of dilutional effects • Aerosol release of botulinum toxin not considered very likely
ILLNESS TYPES AND SYMPTOMS • All naturally occurring types of botulism (infant, food borne, wound and adult intestinal colonization) result in the same illness. • Early botulism: bilateral cranial nerve palsies and descending muscle weakness Symptoms: dry mouth; blurry or double vision; nausea, vomiting or constipation; and difficulty speaking or swallowing. • Late botulism: weakness or paralysis of respiratory muscles may require mechanical ventilation, which can last for months • Incubation Period: • Food borne botulism: 12 – 36 hours • Inhalational botulism (US primate studies): 12 – 80 hours • Case fatality rate: 5% - 10% for food borne botulism. • Lethal Dose: LD50 (amount fatal to 50% of persons exposed) for 154lb person: ~70 micrograms
INCIDENCE • In the United States, an average of 145 cases of botulism are reported each year • 15% foodborne • 65% infant botulism • 20% wound • Adult intestinal colonization and iatrogenic botulism also occur, but rarely • Outbreaks of foodborne botulism involving two or more persons occur most years and are usually caused by home-canned foods • Most wound botulism cases are associated with black-tar heroin injection, especially in California
TREATMENT • Adults/children: botulinum antitoxin • Infants: IV botulinum immune globulin (BIG-IV) antibody injection • Multiple administrations of antitoxin might be needed for persons exposed to higher doses of toxin. • Supportive care, including mechanical ventilation – potentially for months • NO PROPHYLAXIS AVAILABLE
TRANSMISSION, ISOLATION & QUARANTINE • No person-to-person transmission. Isolation not required and quarantine would not be used.
ENVIRONMENTAL STABILITY • Heating food/beverage to boiling for 10 minutes inactivates toxin. Depending on concentration, pasteurization might inactivate most, but not all, toxin • Toxin would be stable on countertops/other environmental surfaces that came in contact with contaminated food item (e.g., spilled milk) • Proper disposal of contaminated food item and decontamination of locations/surfaces where contaminated food item was found
FOOD SAFETY, DECONTAMINATION & REMEDIATION • Once identified, the implicated food item would be collected, disposed and recalled by the manufacturer. • Personal decontamination and bagging/disposal of clothing would not be necessary. • Goals and standards for environmental decontamination will be determined by environmental hazard and risk assessments in collaboration with other agencies.
RE-OCCUPANCY • Limited evacuation, remediation and re-occupancy may be indicated.
PET & VETERINARY • Dogs, cats and sheep: not susceptible to toxins A, B, E or F • Horses/cattle: Susceptible to toxin B • Ferrets: Susceptible to toxins A and E • Birds: Susceptible to toxin E
MENTAL HEALTH IMPACT • Widespread anxiety and distress • Fear driven behaviors (e.g., flight) • Resistance to public health measures
GENERAL CONSIDERATIONS • Multiple attacks possible • Cross-contamination of persons, property, animals and food might occur • Impacts will depend on the nature of the attack(s) and targeted industry and/or populations • Emergency responders who collect food from residences will assume that the environment they are entering is contaminated and will require specific training and equipment • Highly unlikely that MTA would suspend all or parts of service on rail and bus lines
HEATHCARE CONSIDERATIONS • NYC has ~20,000 hospital beds; typically operating at ~80% capacity. Surge in capacities will be needed within 2 days of a large release • Botulism outbreaks have the potential to generate high demand for ICU care (e.g., skilled nursing and ventilators), other staffed beds and mental health services • DOHMH and other ESF 8 partners may need to determine resource allocation strategies and implementation. • Initial symptoms may be vague (e.g., blurred vision). May need nurse’s hotline to triage calls from 311.
HEATHCARE CONSIDERATIONS (continued) • Many persons will go to outpatient offices and emergency departments for evaluation and prophylaxis • Triage methods will be needed to distinguish between those who do and do not need evaluation in emergency departments • Limited supply of antitoxin in the SNS • In an event that involves a widely distributed food product, NYC might be competing with other states for this and other resources • CA Department of Public Health is sole supplier of BIG-IV • Outreach will be needed to both pediatric and internal medicine communities
Past Events • 1971 – Vichyssoise • New York man died and his wife became seriously ill due to botulism after eating a can of Bon Vivant vichyssoise soup • Company began a recall of 6,444 cans of vichyssoise soup made from the contaminated batch • FDA discovered that the company’s processing practices raised questions about all products packed by the company, and subsequently shut down the Newark, NJ plant • Bon Vivant filed for bankruptcy within a month of the announcement of the recall • 1987 - Dried Fish • 8 cases of botulism (2 in New York City and 6 in Israel) from consumption of Kapchunka, an uneviscerated, dry-salted, air-dried, whole whitefish • Product was made in New York City and some of it was transported by individuals to Israel • All 8 patients with botulism developed symptoms within 36 hours • 1 died, 2 required breathing assistance, 3 treated with antitoxin, and 3 recovered spontaneously • 1989 - Bottled Garlic • Bottled, chopped garlic-in-oil mix was responsible for three cases of botulism in Kingston, N.Y. • Two men and a woman were hospitalized • 1992 – Whitefish • Four members of a Fort Lee family were stricken with botulism after eating fish bought in Jersey City • 2007 – Chili Sauce • Botulism found in cans of Castleberry's, Austex and Kroger brands of chili sauce. • Over 25 different brands of a variety of products were recalled • 2010 – Frozen Fish • A New York importer is recalling uneviscerated frozen fish from Vietnam after an inspection found that it might be contaminated with botulism
POTENTIAL DOHMH REQUESTS: TREATMENT ASSETS • Timing and quantity of botulinum anti-toxin • Mechanical ventilators and support equipment • Assistance procuring BIG-IV from CA Department of Public Health (sole supplier)
POTENTIAL DOHMH REQUESTS: Environmental Response Guidance & Standards • Federal assistance in collecting and analyzing environmental samples in coordination with local environmental sampling efforts: • USDA/FSIS: meat, poultry and eggs • FDA: all other food items • Coordination of data sharing requirements • Federal (CDC NIOSH and EPA) and NYSDOH participation in multiagency advisory group for environmental recovery, remediation and re-occupancy issues • Decontamination, remediation and re-occupancy standards and guidelines for locations where contaminated food item was manufactured, stored, prepared and consumed
POTENTIAL DOHMH REQUESTS: Public Health Surge Capabilities • Laboratory sampling and analytical capacity, including staff, reagents and other laboratory supplies (e.g., bioassay, if needed)
POTENTIAL DOHMH REQUESTS:Federal Health/Medical Assets Request from below or order per specific mission needs through ESF-8 via OEM to NY State • National Medical Response Team (medical care; biological incident specialty; mass casualty decon; 50-person, 48 hours; currently one team available for deployment) • Federal Medical Station (acute, non-trauma care; 250 beds scalable in 50 bed increments, 48 hours, order with or without staff; 60 caches around country.) • HHS Rapid Deployment Force (canstaff medical station; clinical; mental health, public health; 105 members, 12 hours; only one available on eastern seaboard) • Pediatric intensivist strike teams (two persons/team; available through Public Health Service Tier III or NDMS.) • Applied Public Health Teams (PHS officers w/ equipment to surge all key local health department functions.) • NDMS Disaster Medical Assistance Teams (Can be configured as needed; approximately six - 35 member teams within a 12 hour deployment zone.