Endocrine System: Overview, hypothalamus and pituitary
450 likes | 1.65k Vues
Endocrine System: Overview, hypothalamus and pituitary. Lecture 41 Tuesday, April 10, 2007 Refs. Ross Chapter 21, Wheater’s Chapter 17, Ganong Chapters 14 and 22, Medical Physiology 46 and 47, Basic Pathology Chapter 20. Endocrine glands and hormones.

Endocrine System: Overview, hypothalamus and pituitary
E N D
Presentation Transcript
Endocrine System: Overview, hypothalamus and pituitary Lecture 41 Tuesday, April 10, 2007 Refs. Ross Chapter 21, Wheater’s Chapter 17, Ganong Chapters 14 and 22, Medical Physiology 46 and 47, Basic Pathology Chapter 20
Endocrine glands and hormones • A hormone is a chemical mediator that reaches its target via the blood stream. • Hormones may act on nearby cells or distant cells. • The glandular tissue secreting hormones does not have ducts. • Endocrine tissue has many capillaries both for blood and lymph. • The endothelium of capillaries is often fenestrated.
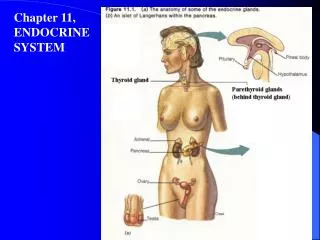
Overview of endocrine tissues and hormones • Hypothalamus many releasing hormones • Pituitary direct acting and trophic • Thyroid gland T3, T4, and calcitonin • Parathyroid glands parathormone • Adrenal glands steroid hormones • Pancreatic islets insulin, glucagon, etc. • Pineal gland melatonin • Neuroendocrine cells many peptides, etc. • Testis androgens • Ovary and placenta estrogen and progesterone
Pituitary or hypophysis • Attached to base of brain beneath the third ventricle in sella turcica. • Secretes 2 functional types of hormones: • Hormones that act on non-endocrine tissue • Prolactin, growth hormone, oxytocin, ADH, and melanocyte stimulating hormone (MSH) • Trophic hormones that alter the secretion of other endocrine glands • Thyroid stimulating hormone (TSH), Luteinizing hormone (LH), adrenocorticotrophic hormone (ACTH), follicle stimulating hormone (FSH). Growth hormone can also have a trophic effect on some endocrine tissues.
Three parts of the pituitary • Neurohypophysis (pars nervosa; posterior pituitary) • Terminal axons of the supraoptic nucleus and paraventricular nucleus store ADH and oxytocin. • Adenohypophysis (anterior pituitary) • derived from the epithelium of the primitive oral cavity • Secretes both direct acting and trophic hormones • Pars intermedia • Remnants of Rathke’s pouch form cysts. • Secretes MSH in some species.
Formation of the anterior and intermediate lobes of the pituitary from Rathke’s pouch Ganong
Control of pituitary gland • Hypothalamus controls secretion of pituitary hormones. • Hypothalamus responds to nervous stimuli from higher centers in the brain and to circulating levels of hormones secreted by pituitary-dependent glands. • Portal system carries hypothalamic releasing hormones to pituitary.
Adenohypophysis H&E stain 480 x WFH 17.3aChromophils stain with H&E, but chromophobes have pale cytoplasm.
Anterior pituitary with stain that makes acidophils orange and basophils blue480 x WFH 17.3b
Anterior pituitary stained with an antibody against LH. 150 x WFH 17.3c
Distribution of cells in adenohypophysis • Somatotrophs 50% growth hormone • Mammotrophs 20% prolactin • Corticotrophs 20% ACTH • Thyrotrophs 5% TSH • Gonadotrophs 5% FSH and LH • Cells are in clusters, mixed, but not evenly distributed throughout the gland.
Pituitary gland. Cells can be identified by size and density of secretory vesicles. TEM 4270 x WFH 17.3d
Neurohypophysis 200 x WFH 17.5aPituicytes are supporting cells similar to neuroglia
Neurohypophysis stained with antibody against neurofilament protein found in axons.Pituicytes (similar to neuroglial cells) do not have neurofilament protein. 100 x WFH 17.5b
Physiology of pituitary gland • Functionally the pituitary is 2 (or 3) endocrine glands. • 1. Posterior pituitary (neurohypophysis or pars nervosa) • Neurons in hypothalamus have axons that extend into posterior pituitary. • Hormones are made in cell body and stored in axons • Supraoptic nucleus- ADH or vasopressin • Paraventricular nucleus- oxytocin • Both are nonapeptides (9 amino acids) • 2. Intermediate lobe (pars intermedia) • 3. Anterior pituitary (adenohypophysis)
Neurosecretion • Neurosecretion- term used to describe secretion of hormones released in response to electrical activity in the neuron. • Actually all neurons secrete chemical mediators, but usually into synaptic cleft. • Difference is that thesesecretions are transported by blood • Neurohormones- hormones secreted by neurons, e.g. ADH, oxytocin, releasing hormones
Vasopressin (antidiuretic hormone) • Has many effects • Antidiuresis-makes collecting duct in kidney permeable to water • Causes insertion of aquaporins into apical membrane of tubule cell. • Water diffuses into hypertonic medulla and urine becomes concentrated. • Stimulates smooth muscle contraction • Contraction of smooth muscle in arterioles increases blood pressure • Intestinal smooth muscle contraction increases peristalsis • Induces uterine contraction
Stimuli for secretion of vasopressin • Increased plasma osmolality (usual physiologic stimulus) • Osmoreceptors in anterior hypothalamus • Outside blood-brain barrier • Blood volume depletion • Pressure receptors in both arteries and veins • Hemorrhage is a potent stimulus for secretion.
Diabetes insipidus • Clinical signs • Polyuria- production of large volumes of dilute urine due to inability to concentrate urine • Polydipsia-ingestion of large volumes of fluid-necessary to prevent dehydration • Causes • Central- lack of ADH secretion • Nephrogenic- lack of renal response to ADH • Treatment for central diabetes insipidus • Exogenous ADH either intranasal or parenteral injection
Anterior and intermediate pituitary • Both are derived embryologically from Rathke’s pouch, an evagination of the epithelium of the roof of the pharynx. • Intermediate lobe is rudimentary in humans. • Secretes melanocyte-stimulating hormone (MSH) in some species • Usually involutes during childhood; MSH not secreted normally in adults. • Adenohypophysis secretes 6 hormones. • see Ganong fig 14-16; function of b-lipotropin is unknown. • Both direct-acting or trophic hormones • Some cells in both lobes express the same pre-prohormone precursor pro-opiomelanocortin (POMC). • Intermediate lobe processes it to MSH, CLIP. • Corticotropes hydrolyze it to ACTH and bLPH.
Processing of pre-pro-opiomelanocortin. AL anterior lobe, IL intermediate lobe. Ganong 22-2 Similar to MP 49-4.
Control of adenohypophysis • Hypothalamus controls secretion of anterior pituitary by secreting releasing and inhibiting hormones. • Portal system: Capillaries around ventral hypothalamus drain into portal veins and carry high concentrations of releasing hormones to the hypothalamus but very little reaches the general circulation.
Summary of hypophysiotropic hormones. Note that the hypothalamus also produces inhibitory hormones. Ganong
Acronyms of hypophysiotropic hormones • CRH corticotropin-releasing hormone • TRH thyrotropin-releasing hormone • GnRH gonadotropin-releasing hormone • GRH growth hormone-releasing hormone • GIH growth hormone-inhibiting hormone = somatostatin • PIH prolactin-inhibiting hormone • PRH prolactin-releasing hormone, postulated
Growth hormone • Acts both directly on target tissues and as a tropic hormone by stimulating production of a family of growth hormones including insulin-like growth hormones I and II in liver and other tissues • Growth hormone has many effects usually with IGF. • Chondrogenesis- formation of cartilage • If growth plates have not closed, GH causes giantism. • When epiphyses are closed, GH causes acromegaly
Growth hormone con’t • Anabolic • Increase in protein mass. • Lipolytic- decrease in body fat. • Pituitary release of GH is controlled by GRH and somatostatin secretion by the hypothalamus
Control of growth hormone secretion.Growth hormone stimulates liver and other tissues to make insulin-like growth factor (IGF-I) Ganong
Physiology of growth • Complex phenomenon • Other hormones involved- thyroid hormones, androgens, estrogens, glucocorticoids, insulin, insulin-like growth factor • Genetic factors • Nutrition • 2 periods of rapid growth in humans: • Infancy • Puberty (estrogens induce epiphysial closure)
Types of endocrine disease • Underproduction of hormone • Lack of trophic hormones • Destructive processes ( ischemia, radiation, inflammation) • Overproduction of hormone • Clinical signs depend on the hormone in excess • Mass lesions • Benign adenomas or invasive carcinomas • Can cause overproduction of hormone (functional) • Can cause decreased production of hormone (nonfunctional)
Diseases of the adenohypophysis • Any endocrine cell type can become an adenoma • Usually functional adenomas are diagnosed by the endocrine abnormality they cause. • Prolactinomas- infertility; inappropriate milk secretion • most common • Corticotroph adenomas secrete ACTH causes Cushing’s syndrome • Death can be caused cardiac and metabolic effects of cortisol • Somatotroph adenoma- excess growth hormone can cause gigantism or acromegaly • Thyrotroph and gonadotroph adenomas are rare.
Pituitary adenomas • Non-secreting adenomas are often large when diagnosed • Signs are due to pressure on surrounding structures • Visual disturbances due to pressure on optic chiasm • Bitemporal hemianopsia • Hypopituitarism due to destruction of functional pituitary • Pituitary apoplexy occurs when pituitary suddenly increases in size e.g. hemorrhage into adenoma.