Download
1 / 39
390 likes | 440 Vues
Learn about osteoporosis, its risk factors, clinical signs, diagnostic methods, and treatment guidelines to help manage this bone disorder effectively.

E N D
INTRODUCTION — Osteoporosis is the most common bone disease. • DEFINITION — Osteoporosis is a skeletal disorder characterized by two elements: • low bone mass • and microarchitectural disruption.
There are fewer bony spicules in osteoporotic bone and they are thinner • But the bone that is present is normally mineralized,
EPIDEMIOLOGY • It is estimated that over 1.3 million osteoporotic fractures in the United States. • One-half are vertebral fractures, • One-quarter are hip fractures, • And one-quarter are Colles' fractures. • Among subjects age 90 years, 33 percent of women and 17 percent of men will have a hip fracture . • After age 50 years, a woman is three times more likely than a man to have a vertebral or hip fracture
Risk Factors For Osteoporosis: • Age. • Sex. • Organs Failure. • Certain drugs include glucocorticoids, heparin, cyclosporine, medroxyprogesterone acetate, vitamin A and certain synthetic retinoids, Anxiolytic, anticonvulsant, or neuroleptic drugs. • Organ transplantation . • Cancer treatment. • Vitamin B12 deficiency
Previous fracture between the ages of 20 and 50. years • History of fracture in a first degree relative. • Cigarette smoking . • Inflammatory bowel disease. • Sedentary life style. • Consumption of large amounts of caffeine. • Above average height. • Low body weight or weight loss. • Type 2 diabetes mellitus .
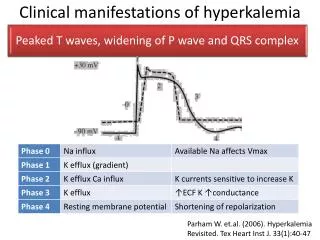
Clinical Manifestations • Osteoporosis has no clinical manifestations until there is a fracture. • many patients with achy hips or feet do not have osteoporetic fractures but they have osteomalacia . • Vertebral fracture • Vertebral fracture is the most common • Most of these fractures (about two-thirds) are asymptomatic;
Osteoporotic fracture can lead to the acute onset of pain. Successive fractures lead to increased thoracic (dorsal) kyphosis with height loss "dowager's hump“ and complain of "getting fat" without any change in weight. Their abdomen becomes protuberant. The distance from the occiput to the wall (normally 0 cm). The size of the gap between the costal margin and the iliac crest (normally three finger breadths).
Other fractures • Hip fractures are relatively common in osteoporosis, affecting 15 percent of women and five percent of men by 80 years of age. • RADIOGRAPHIC FEATURES • Plain radiographs show detectable changes when bone loss exceeds 30 percent. • An early manifestation is "codfish" vertebrae.
DIAGNOSIS • MEASUREMENT OF BONE DENSITY: • Several different methods are used to measure bone density : • Single-photon absorptiometry;wich can be used only at peripheral sites (radiusand calcaneus). • Dual-photon absorptiometry (DPA) that measure bone density at the spine and hip
Dual x-ray absorptiometry(DEXA): • The two photons are emitted from an x-ray tube instead of a radioactive source. • DXA is the most popular method for measuring bone density at the spine and hip and some times at distal of radious bone.
Ultrasonography • Potential advantages include lower expense, portability, and lack of radiation exposure. • Measurements are usually made at the patella or calcaneus (heel). • Quantitative ultrasound is a good predictor of fracture risk especially in pregnancy. • A major limitation to using is that the criteria for diagnosing osteoporosis and recommending treatment are not yet well established.
Every Patient Spine L2-L4 Hip Total Proximal Femur Osteoporosis Femoral Neck Trochanter Some Patients Forearm (33% Radius) If hip or spine cannot be measured Hyperparathyroidism Very obese Which Skeletal Sites Should Be Measured? Use lowest T-score of these sites
Indications For Bone Density Testing • All women age 55 and older • All men age 65 and older • Adults with a fragility fracture • Adults with a disease or condition associated with low bone density • Adults taking medication associated with low bone density • To monitor treatment effect
DEFINITIONS • Osteopenia • Bone mineral density (BMD) measurement at any site > 1 but 2.5 standard deviations below the young adult standard • T score < -1 but -2.5
Definitions • Osteoporosis • BMD measurement at any site > 2.5 standard deviations below the young adult standard with or without previous fracture • T score of < -2.5
Diagnostic Classification WHO Study Group. 1994.
SCREENING FOR SECONDARY CAUSES Disease Recommended Laboratory Tests (boldeditems are recommended routinely) Cushing’s disease Electrolytes, 24-hour urinary cortisol Hyperthyroidism TSH, T4 Hypogonadism Bioavailable testosterone Multiple myeloma CBC, serum electrophoresis, urine electrophoresis Osteomalacia Alkaline phosphatase, 25(OH)D Paget’s disease Alkaline phosphatase Primary hyperparathyroidism Calcium, PTH
Treatment Guidelines Summary of recommendations for pharmacologic therapy according to T-score from the National Osteoporosis Foundation (NOF) and the American Association of Clinical Endocrinologists (AACE) † Fragility fracture, family history of fracture, cigarette smoking, low body weight (<127 lbs.), etc.
RISK FACTORS FOR POSTMENOPAUSAL WOMEN • Early menopause • White or Asian race • Sedentary life style • Smoking • Small frame • Alcohol abuse • Primary hyperparathyroidism • Hyperthyroidism • Glucocorticoid use
CALCIUM & VITAMIN D • Calcium and vitamin D maintain or increase bone density & help prevent hip and nonvertebral fractures • Men 65 years and older & postmenopausal women should ingest a total of 800 IU of vitamin D and 1200 mg / day of calcium daily. • Higher doses are required if they have malabsorption or rapid metabolism of vitamin D
Estrogen/progestin therapy • Estrogen-progestin therapy is no longer a first-line approach because of Increased risk of : • Breast cancer, • Stroke, • Venous thromboembolism, • And perhaps coronary disease. • HRT Prevents bone loss at hip & spine when initiated within 10 years of menopause
Possible indications for estrogen-progestin in postmenopausal women include persistent menopausal symptoms and… • women with an indication for antiresorptive therapy who cannot tolerate the other drugs or because of side effects. • There was a significant 33 percent reduction in clinical vertebral fractures and a 23 percent reduction in other osteoporotic fractures.
Bisphosphonates • Alendronate (10 mg/day or 70 mg once weekly) or risedronate (5 mg/day or 35 mg once weekly), are good choices for the treatment of women with established osteoporosis. • These drugs increase bone mass and reduce the incidence of vertebral and nonvertebral fractures (even in women who already have fractures).
The beneficial effects of alendronate persist over several years after treatment is stopped, • When given, alendronate or risedronate should be taken with precautions to avoid pill-induced esophagitis. • Alendronate appears to be well tolerated and effective for at least ten years .
Residronate (Actonel) Approved for osteoporosis prevention & treatment of osteoporosis: 5 mg / day In comparison with placebo: bone density of spine & hip new vertebral fracture rate GI side effects Zolindronic acid(Aclasta) Only infusible drug approved for treatment of osteoporosis and the most strong members. Use for idiopathic osteoporosis only if other treatments are ineffective or conterindicated. OTHER BISPHOSPHONATES
SELECTIVE ESTROGEN RECEPTOR MODULATORS (SERMs) • Act as estrogen agonists in bone and heart. • Act as estrogen antagonists in breast and uterine tissue • Potential for preventing osteoporosis without the increased risk of breast or uterine cancer
Rationale Approved for osteoporosis prevention & treatment in postmenopausal women In comparison with placebo: vertebral fractures by 60% breast cancer (relative risk 0.24) bone turnover & maintained hip & total body bone density total cholesterol and LDL levels Side effects Flu-like symptoms, hot flushes, leg cramps Peripheral edema SERMs: RALOXIFENE
Calcitonin • A less popular choice for treatment of osteoporosis is nasal calcitonin, 200 IU/day. • It is a weak drug for treatment and because of tachyphylaxis has a little effect on density. • There is one exception,most use calcitonin as first-line therapy in patients who have substantial pain from an acute osteoporotic fracture. • Dosing • Subcutaneous injection • Nasal spray (fewer reported side effects,
Monitoring of treatment • Bone density measurement can be repeated after one year of therapy. • If BMD is stable or improving, that would be evidence for treatment response. • However, if BMD declines at one year, compliance with drug, calcium and vitamin D should be verified, and some evaluation for secondary causes of bone loss should be performed . • If the patient is otherwise well and taking the drug and supplements correctly, the correct action is controversial.
Some physicians believe that the decrease in BMD truly reflects a treatment failure and would consider modification of the primary treatment for the osteoporosis. • Others believe that the decline in BMD is not necessarily reflecting inadequate therapy, but could be ascribed to measurement error and would repeat BMD one year later, taking action only if the decline is reaffirmed.