Download
1 / 6
100 likes | 1.02k Vues
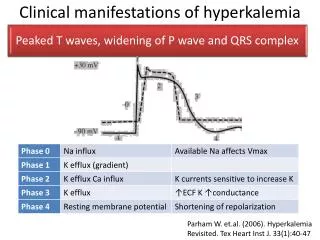
Clinical manifestations of hyperkalemia. Parham W. et.al. (2006). Hyperkalemia Revisited. Tex Heart Inst J. 33(1):40-47. Clinical manifestations of hyperkalemia. hyperkalemia partially depolarizes the cell membrane.

E N D
Clinical manifestations of hyperkalemia Parham W. et.al. (2006). Hyperkalemia Revisited. Tex Heart Inst J. 33(1):40-47
Clinical manifestations of hyperkalemia • hyperkalemiapartially depolarizes the cell membrane. • Prolonged depolarization impairs membrane excitability and is manifest as weakness, which may progress to flaccid paralysis and hypoventilation if the respiratory muscles are involved
Clinical manifestations of hyperkalemia Metabolic Acidosis • Hyperkalemia inhibits renal ammoniagenesis and reabsorption of NH4+ in the TALH • Net acid excretion is impaired and results in metabolic acidosis =15 Hyperglycemia400 mg/dL (300≈DKA) Acid anion - acetoacetate
Management • Calcium gluconate↓membrane excitability • 10 mL of 10% solution infused over 2-3 min • Effect seen ECG after 5-10 min (if not-repeat dose) • Insulin for K+ shift into cells • 10-20 units regular insulin • Fall by 0.5-1.5 mmol/L in 15-30 min
Management (DKA) • Replace fluids: • 2-3L of 0.9% saline over first 1-3h; • subsequently, 0.45% saline at 150-300 mL/h; • change to 5% glucose and 0.45% saline at 100-200mL/h when plasma glucose reaches 250 mg/dL • Short-acting insulin:IV (0.1 u/kg) • then 0.1 u/kg/h by continuous IV infusion • Monitor glucose q1-2h • electrolytes, anion gap q4h for 1st 24 h • Glucose goal is 150-250 mg/dL • insulin dec 0.05-0.1u/kg/h
Management • Dialysis • Intractable acidosis • Intractable electrolyte imbalance • Intoxication • Intractable volume overload • Intractable uremia