VAP Ventilator-Associated Pneumonia
350 likes | 1.87k Vues
VAP Ventilator-Associated Pneumonia. By: Erika Rodriguez RN, BSc Shanay Jackson RN Stephen Jaime RN, BSc Mykell Johnston RN, BSc Ashley Valencia RN, BSc Mayra Valenzuela RN, BSc. Ventilator Associated Pneumonia. VAP is defined as :

VAP Ventilator-Associated Pneumonia
E N D
Presentation Transcript
VAPVentilator-Associated Pneumonia By: Erika Rodriguez RN, BSc Shanay Jackson RN Stephen Jaime RN, BSc Mykell Johnston RN, BSc Ashley Valencia RN, BSc Mayra Valenzuela RN, BSc
Ventilator Associated Pneumonia VAP is defined as: • Acute inflammation of lung parenchyma caused by an infectious agent • A subset of Hospital Acquired Pneumonia (HAP) • Occurs > 48 hours after intubation (Urden, et. al, 2006)
The Practice Problem • Patients intubated >24 hours are 6-21 times more likely to develop VAP than those intubated less than <24 hours • Incidence rate: 20-65% • VAP increases: • ventilator days by 4 • critical care days by 4 • hospital lengths of stay by 9 days • VAP mortality rates are 20-41% • The Bottom Line: Can increase costs by $50,000 (AACN, 2008)
Previous Practice • Nursing staff failed to routinely integrate oral care and suctioning for patients on mechanical ventilation. • Failure to perform frequent and consistent oral care and suctioning had resulted in an increased incidence of VAP.
PICO In ventilator dependant patients does oral care and suctioning using high-low, closed-suction and oral suction lower the incidence of ventilator associated pneumonia?
Innovation/Intervention For patients on a mechanical ventilator: Initial Ventilator Orders @ ECRMC • Keep HOB elevated at 30-45 degrees if hemodynamically stable • Oral Care every 4hrs per policy • ET aspirate post-intubation (before antibiotics) & again in 3 days post intubation • Non-Diabetic pts- daily AM blood sugar, notify MD if glucose >120 • Diabetic pts- capillary blood glucose Q6hrs, sliding scale • Hold sedation daily each morning with neurological assessment
Literature Review • Colonization of the oropharynx is a critical factor in developing nosocomial pneumonia (Muncro & Grap (2004) • Dental plaques provide a habitat for micro-organisms that can travel to the lungs & colonize (Fourrier, et. Al, 1998) • Dental plaque can be removed by brushing (ADA, 2006) • The ADA recommends brushing twice daily to remove plaque from all tooth surfaces (ADA, 2006) • The use of an oral care protocol reduces oral inflammation & improves oral health (Fitch, et. Al (1999)
Objectives Decrease VAP by the following methods: • Educate RN’s on the significance of VAP & oral care protocol using the AACN Practice Alert (2008) • Improve performance & documentation of oral care frequency including oral care (brushing) and oral cavity moisturizing
Implementation • Protocol developed by VAP team consisting of RTs and RNs from all nursing departments • Protocol developed after reviewing research from VHA & IHI • Provision of supplies in ICU for oral care and ETT with Hi-Low suction • Nursing education in the ICU • Include the oral care procedure as part of unit orientation to ensure consistency of care • Documentation verification • Watching VAP trends in the ICU
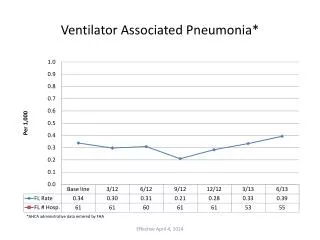
Results • August 2007: oral care and moisturizing, use of ETT with Hi-Low suction, oral suctioning and in-line suction, HOB elevation, protocol initialed • Decrease in VAP cases @ ECRMC 2006: 8 VAP cases 2007: 5 VAP cases 2008: 3 VAP cases 2009: 0 VAP cases
SWOT Analysis • Strengths • Simplicity of the intervention • Lack of reimbursement • Cost effective • Weakness • Limited clinical studies • ER failure to obtain 1st sputum sample • Opportunities • High mortality • Cuts LOS • Cuts cost • Threats • Requires diligence • Prolonged ventilation • Additional risk factors
Future Implications • There is need for a large, well-controlled clinical trail of oral care interventions in critical care patients separate from the chlorhexidine studies • Ensure use of an ETT with a dorsal lumen above the endotracheal cuff to allow drainage by continuous suctioning of tracheal secretions that accumulate in the subglottic area (Tablan, et. al., 2004) • Patients requiring intubation > 7 days would benefit from an early tracheostomy. Evidence shows VAP incidence is 42.3% on late tracheostomies versus 27.2% on early tracheostomies (p<0.05) (Tablan, et. al., 2004) • Incorporate higher vigilance with patients who have other risk factors for VAP
Future Implications • ECRMC is currently looking at trends/ problem areas • Pts intubated by EMS. EMS is currently not using ETT with Hi-Low suction • Pts transferred from Mexicali Vent days > 48hrs • Reviewing Weaning protocol
VAP: Additional Risk Factors • Decreased level of consciousness • Supine positioning with HOB flat • Use of H2 antagonists and antacids • Gastric distention • Presence of gastric or small intestine tubes • Enteral feedings • Trauma • COPD (AACN, 2008)
ANALYSIS OF BEST PRACTICES According to AACN (2008), the best nursing practices in preventing VAP effectively are a combination of: • Good hand washing techniques • HOB elevation (30-45 degrees) • Brushing of teeth, gums & tongue at least twice daily • Oral moisturizers q 2-4 hours • Nasal, oral, and subglottal suctioning (high-low & deep suctioning included) • The use of chlorhexidine oral rinse for perioperative cardiac surgical patients • Daily sedation vacation
References AACN Practice Alert (October, 2007). Oral Care in the Critically Ill. AACN Practice Alert (January, 2008). Ventilator Associated Pneumonia. American Dental Association. (September 19, 2006). Oral Health Topics: Cleaning your teeth and gums. Fitch, et. al. (1999). Oral care in the adult intensive care unit. American Journal of Critical Care. 8:314-318. Fourrier, et. Al (1998) Colonization of dental plaque: a source of nosocomial infections in intensive care unit patients. Critical Care Medicine. 26:301-308 Munro & Grap. (2004). Oral health and care in the intensive care unit: state of the science. American Journal of Critical Care. 13:25-33. Tablan, et. al. (2004). Guidelines for preventing healthcare-associated pneumonia, 2003: recommendations of CDC and the Healthcare Infection Control Practices Advisory Committee. MMWR. 53(RR-3):1-36. Urden, et. Al. (2006). Thelan’s Critical Care Nursing: Diagnosis and Management, 5th ed. Mosby. Missouri.