Download
1 / 31
310 likes | 327 Vues
Learn about anticoagulation tests for heparin on mechanical circulatory support and methods to resolve discrepancies between tests. Explore the role of activated partial prothrombin time, unfractionated heparin anti-Xa, and antithrombin. Understand thromboelastography and its relevance in monitoring hemostasis.

E N D
Noncardiac Sources of PainAnticoagulation in the CICUConflict Amongst Coagulation Tests Jonny Byrnes MD CICU Attending Cincinnati Children’s Hospital Medical Center Assistant Professor University of Cincinnati Jonathan.byrnes@cchmc.org
I have no financial disclosures. • Antithrombin concentrates/ recombinant antithrombin is not FDA approved for the replacement on mechanical circulatory support.
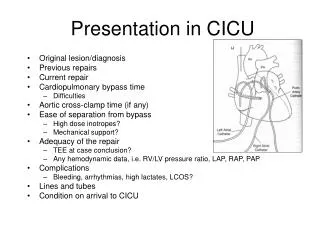
Objectives Review typical anticoagulation tests in context of heparin anticoagulation on MCS Methods to resolve discrepancy between tests Cases
Laboratory Monitoring Activated partial prothrombin time Unfractionated Heparin anti-Xa Antithrombin Thromboelastography
Activated Partial Prothrombin Time (aPTT) Laboratory test typically used to monitor heparin therapy. Different reagents used may influence results, so lab specific ranges. Typically therapeutic is considered levels 1.5-2.5 normal range.
aPTT • The tube contains a calcium binder to arrest coagulation • Calcium, an activator, and a phospholipid are added to start coagulation in the lab. • The aPTT is the number of seconds it takes to initiate thrombus formation. • aPTT assays vary based on reagents used, so value can not necessarily be compared amongst labs.
Abnormalities of the aPTT • Shortened aPTT is typically thought to be of little consequence • Prolonged aPTT • Lupus anticoagulant/antiphospholipid antibody • Hemophilia • DIC • Factor inhibitors • Deficiency of factors VIII, IX, XI, XII
Unfractionated Heparin anti-Xa level • Addition of known amounts of factor Xa and antithrombin added to the sample. • UH forms an inhibitory complex with antithrombin and inactivates factor Xa. • Excess factor Xa remaining is inversely proportional to the original amount of UH. • Compared to a standard curve and a concentration of anti–factor Xa is estimated.
Unfractionated Heparin anti-Xa level • As described is functionally a heparin level • Since exogenous AT is added at most institutions may not represent physiologic anti-Xa level • Therapeutic ranges • UF 0.3-0.7 IU/ml • Low level: consider improper collection, nontherapeutic dosing, or delay in separating plasma. • High Level: heparin contamination from line or renal impairment.
Unfractionated anti-Xa level Nankervis, 2007
Antithrombin level Heparin Mechanism AT Thrombin Xa 1000 x Heparin
Antithrombin • Developmental variation • Initially 40-70% in newborn period • Adult levels of 80-120% by 2 years of age • Deficiency • Congenital • Acquired: DIC, Sepsis, Protein Losing Conditions, Liver Disease • Replacement
TEG Technology:How It Works • Cup oscillates • Pin is attached to a torsion wire • Clot binds pin to cup • Degree of pin movement is a function of clot kinetics • Magnitude of pin motion is a function of the mechanical properties of the clot Slide courtesy of Haemoscope company
Thromboelastography • Whole blood, POC test • Measures hemostasis – clot initiation thru lysis • Net effect of and interaction of different hemostatic components
Thromboelastogram LY30 Amount (%) of fibrinolysis or clot contraction occurring 30 minutes after the point of maximal amplitude α-angle Interaction between fibrin and platelets Clot MA Total clot strength, overall platelet strength R value Initiation of a white clot, can represent extrinsic, intrinsic, or common pathway 0 10 20 30 40 50 60 70 Nml 5-10 55-73 47-74 0-8% R value 8.6 MA 61 α-angle 58 4.1% LY30
This is your TEG This is your TEG on heparin CKH CK nml R value 8 19 5-10 MA 61 28 55-73 α-angle 58 34 47-74 LY30 2 5 0-8% 10 10 20 20 30 30 40 40 50 50 60 60 70 70
Possible Scenarios of Conflict/Disagreement UF Heparin anti-Xa is supratherapeutic, aPTT, and TEG are normal/subtherapeutic. aPTT is supratherapeutic, UF Heparin anti-Xa and TEG are therapeutic/subtherapeutic. TEG R is supratherapeutic, aPTT and UF Heparin anti- Xa are therapeutic/subtherapeutic.
Possible Scenarios of Conflict/Disagreement aPTT and TEG R are supratherapeutic, UF Heparin anti-Xa is therapeutic/subtherapeutic TEG heparinase R appears short with adequate heparin, aPTT & UF Heparin anti-Xa is therapeutic.
Possible Scenarios of Conflict/Disagreement UF Heparin anti-Xa is supratherapeutic, aPTT, and TEG are normal/subtherapeutic. This scenario is the most straightforward and typically will be related to contamination from the line. In any patient on mechanical support it is useful to remove all heparin from one of the lines for lab draws so that there is no risk of contamination.
Possible Scenarios of Conflict/Disagreement aPTT is supratherapeutic, UF Heparin anti-Xa and TEG are therapeutic/subtherapeutic. This could be related to a lupus “anticoagulant” or anti-phospholipid antibody Commonly seen after a period of turning off the heparin and after heparin is restarted the contact system is activated within the circuit where Factors IX, XI, XII are consumed. - sending specific factor studies for factors IX, XI, XII Possible reagent problem with aPTT assay
Possible Scenarios of Conflict/Disagreement TEG R is supratherapeutic, aPTT and UF Heparin anti-Xa are therapeutic/subtherapeutic. Insufficient coagulation factor production by the liver or consumption - Sending factors V, VII can be helpful. Second anticoagulant such as a direct thrombin inhibitor or coumadin is affecting the coagulation Possible reagent problem with TEG assay
Possible Scenarios of Conflict/Disagreement aPTT and TEG are supratherapeutic, UF Heparin anti-Xa is therapeutic/subtherapeutic Heparinoid from the glycocalyx or from acute liver failure is affecting aPTT and TEG Disseminated intravascular coagulation or lack of production of factors II, V, VII, or X in addition to a lack of factors in the contact system.
Possible Scenarios of Conflict/Disagreement TEG heparinase R appears short with adequate heparin, aPTT & UF Heparin anti-Xa is therapeutic. Inflammation is driving a hypercoaguable state through fibrin and thrombin mediated thrombin generation. - factor VIII level can be considered - fibrinogen level will be high - commonly associated with fevers
Case 1 3 month old, recent ALCAPA dx Day 1 Transthoracic VA ECMO Day 1 for LV recovery after ALCAPA repair, MV annuloplasty Chest tubes clearing, 1-2 cc/kg/hr, no bleeding from lines
Case 1 PT 9 sec aPTT 122 sec UF anti Xa 0.12 u/ml CKH TEG R 8 α 61 MA 62 LY30 4% CK TEG R 11 α 35 MA 42 LY30 8% AT3 84% ACT 150 sec
Case 1 PT 9 sec aPTT 122 sec UF anti Xa 0.12 u/ml CKH TEG R 8 α 61 MA 62 LY30 4% CK TEG R 11 α 35 MA 42 LY30 8% AT3 84% ACT 150 sec
Case 1 Factor IX 32% Factor XI 16% Factor XII 50% 2 Approaches Possible • Give FFP to correct factor deficiency and turn up heparin to prevent further activation of extrinsic pathway. • Wait for liver to correct factor deficiency and turn up heparin now to prevent further activation of extrinsic pathway.
Case 2 4 year old, myocarditis s/p Rotaflow temporary LVAD for cardiogenic shock MCS Day 4, hemodynamically well supported. Intermittent fevers (culture negative for the last 48 hours) Chest tubes clearing, ~1 cc/kg/hr, no bleeding from lines. Heparin 24 u/kg/hr
Case 2 PT 9 sec aPTT 70 sec UF anti Xa 0.35 u/ml CKH TEG R 3 α 75 MA 68 LY30 4% CK TEG R 16 α 35 MA 42 LY30 % AT3 84% ACT 170 sec Fibrinogen 800 mg/dl CRP 8 mg/dl WBC 27K
Case 2 PT 9 sec aPTT 70 sec UF anti Xa 0.35 u/ml CKH TEG R 3 α 75 MA 68 LY30 6% CK TEG R 16 α 35 MA 42 LY30 2% AT3 84% ACT 170 sec Fibrinogen 800 mg/dl CRP 8 mg/dl WBC 27K
Conclusions There is no one “best” anticoagulation test for managing heparin in critically ill patients. Specific coagulation factor testing often proves helpful. Interdisciplinary collaboration is useful when the coagulation tests do not align.