Download
1 / 31
330 likes | 577 Vues
Coagulation-Anticoagulation Balance and Imbalance of Haemostatic System. Clinical Significances of Hemostasis. Bleeding Disorders. Hemophilia A. VIII. Deficiency in vitamin K. von Willebrand disease. Deficiencies in factor IX. Antithrombin deficiency. Thromboembolism. Role of Vitamin K.

E N D
Coagulation-Anticoagulation Balance and Imbalance of Haemostatic System
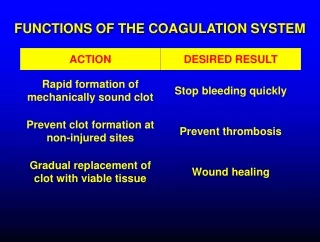
Clinical Significances of Hemostasis Bleeding Disorders Hemophilia A VIII Deficiency in vitamin K von Willebrand disease Deficiencies in factor IX Antithrombin deficiency Thromboembolism
Role of Vitamin K Vitamin K-dependent carboxylase Carboxylated prozymogens Inactive prozymogen (Clotting factors II, VII, IX, X, protein C and S)
Contents • Concepts: Disseminated Intravascular Coagulation (DIC), Shwartzman reaction • Conditions and predisposing factor • Mechanism of DIC • Clinical and laboratory findings • Prevention and treatment principle
Definition A disorder of widespread micro-vascular thrombosis caused by activation of coagulation with or without bleeding caused by secondary fibrinolytic activation.
Case Presentation A 23-year woman, induced abortion, delivered one dead fetus. After parturition, profluvium sanguis from vagina constantly. 14 hrs after parturition, convulsion and obnubilation developed. Large ecchymosis on extremities and abdomen. BP: undetectable; platelet: 7,000; BT: 1 min; CT: 1min; PT: 18 sec; Fib:1.1g/L; 3P test (+)
Conditions Causing DIC Syndromes Infections (most common): Acute DIC: Bacteria and their toxins, fungi, viruses, rickettsiae;Chronic DIC: Any chronic infection (eg, tuberculosis, abscesses, osteomyelitis)Malignancy: Acute DIC: Acute promyelocytic leukemia, acute monocytic leukemia, disseminated prostatic carcinomaChronic DIC: Lung, breast, gastrointestinal malignancy Obstetrical complications: Acute DIC: Abruption placenta, abortions (especially therapeutic abortions), amniotic fluid embolism, hemorrhagic shockChronic DIC: Dead fetus syndromeTrauma:Acute DIC: Massive tissue destruction, brain damage Vascular disease: Acute DIC: Brain infarction or hemorrhageChronic DIC: Aortic aneurysm, giant hemangiomaVenoms: Acute DIC: Snake, spider (rare)Others: Acute DIC: Heparin-induced thrombocytopenia with thrombosis (HITT), purpura in newborns (homozygous protein C deficiency)
DIC Predisposing Factors Impaired clearance system: Liver, mononuclear phagocyte Shwartzman reaction; Hypercoagulable state: e.g., pregnancy; Disorder of microcirculation: e.g., giant hemangioma.
Infection Childbirth, dead fetus, or surgery Cancer Poisonous snake Severe head injury Endothelial damage; tissue damage; director activation of factor X, damage of blood cells Hypercoagulable stage Excessive clotting Hypocoagulable stage Clotting factors and platelets are depleted Secondary fibrinolytic stage Excessive bleeding occurs
Scanning electron micrograph of moderately active platelet Pseudopods
Intrinsic Extrinsic The “Cascade” theory of Coagulation
Anticoagulation System Cells Macrophage, endothelial cell, etc Molecules Serine-containing enzyme inhibitors; Protein C system; Tissue factor pathway inhibitor; Fibrinolytic system, etc
Controls at Thromblin Level Antithrombin III is the most important Others: a2-macroglobulin heparin cofactor II a1-antitrypsin
Protein C Thrombomodulin Thrombin Activated Protein C Protein S Degradation of Va, VIIIa Resistance to activated protein C in patients with thromboembolism
tPA: tissue plasminogen activator; PAI-1: plasminogen activator inhibitor; AP: antiplasmin
VEC TFPI tPA,uPA PAI PC, PS, TM Plasmin Heparin+ATIII FDPS TFPI: tissue factor pathway inhibitor; PC: protein C; PS: protein S; TM: thrombodulin; ATIII: antithrombin III; tPA:tissue plasminogen activator; uPA:urokinase; FDPS: fibrin degradation products; plasminogen activator-inhibitors type 1 (PAI-1);VEC: vascular endothelial cell.
Clinical and Laboratory Findings in DIC Clinical findings • Bleeding at multiple sites (Ecchymoses of skin, mucous membranes; Visceral hemorrhage) • Organ dysfunction (Waterhouse-Friderichsen syndrome; Sheehan’s syndrome) • Shock • Hemolytic anemia(microangiopathic hemolytic anemia)
Integumentary system: Widespread hemorrhage and vascular lesions, Oozing from puncture sites, incision, mucous membranes, irregular-shaped cyanotic patches Central nervous system: Subarachnoid hemorrhage, altered state of consciousness Gastrointestinal system: Occult bleeding to massive gastrointestinal bleeding; abdominal distention; malaise, weakness Pulmanary system Renal system: hematuria, oliguria, renal failure
Laboratory abnormalities • Coagulation abnormalities: prolonged prothrombin time, activated partial thromboplastin time, thrombin time; decreased fibrinogen levels; increased levels of FDP (eg, “3P” test, D-dimer) • Platelet count decreased as a rule but may be falling from a higher level yet still be normal • Schistocyte
Plasma Protamin Paracoagulation Test (“3P”test) FDP+Fibrin Protamin Fibrin Aggregation FDP+Protamin
Treatment Principles Treat the underlying disease 1. Avoid delay2. Treat vigorously (eg, shock, sepsis, obstetrical problems)
Manage the DIC Blood components as needed Fresh frozen plasma Platelet transfusions Anticoagulants after bleeding risk is corrected