Download
1 / 25
250 likes | 275 Vues
Learn about auditory dys-synchrony, clinical manifestations, audiological profiles, and developmental interventions for children with auditory neuropathy. Discover Zachary's journey and successful auditory management strategies.

E N D
Fostering auditory development of a child with auditory neuropathy Holly Gilliam Yusnita Weirather, M.A., CCC-A Deborah Gabe, M.A., CCC-A March 4, 2005
Terminology • Auditory neuropathy • Auditory dyssynchrony • Nonperipheral hearing loss • Hearing loss beyond the cochlea • Sensori-neural hearing loss • Unconventional hearing loss
What is auditory dys-synchrony? • Hearing impairment is a disorder of auditory nerve function and may have, as one of its causes, a neuropathy of the auditory nerve, occurring either in isolation or as part of a generalized neuropathic process (Starr et al, Brain, 119 (3): 741) • A hearing disorder in which sounds enters the inner ear normally but the transmission of signals from the inner ear to the brain is impaired (NIDCD). • A type of hearing loss where the cochlea seems to work, but there is something wrong with how the auditory nerve works (Deafness and Family Communication Center (DFCC) at the Children's Hospital of Philadelphia).
Aidan’s mom • I have read that people with AN can hear in a number of ways. Some hear sound, but not clearly enough to distinguish speech. Some have moments of clarity and moments of dysynchrony. And I’ve even heard of someone whose child could hear relatively clearly for months at a time and then lose that clarity again. That is part of what is so frustrating to me as a new AN mom - there isn’t any definitive answer to what my child is hearing www.raisingdeafkids.org/hearingloss/types/an
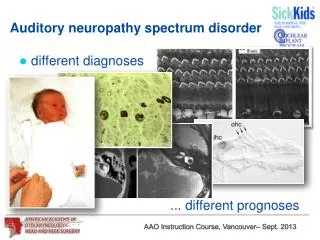
Audiological test results • Presence of cochlear hair cell activity - cochlear microphonics in ABR - otoacoustic emissions (may later disappear) • Absence of auditory nerve response - no ABR wave forms observed • Behavioral audiometric test results vary - fluctuating responses - audiograms range from normal to profound
Clinical manifestations • Ability to detect sounds and speech cannot be predicted by ABR results. • Pure tone audiogram becomes important to determine what the child hears. • Word recognition ability is worse than predicted by the pure tone audiogram. • Functional hearing ability changes and cannot be predicted and occasionally, in the long term, hearing may improve • Hearing aid benefits are not uniform across cases
Zachary’s audiological profile • Failure of bilateral newborn hearing screening with ABR • Absent auditory brainstem responses to click stimuli at a 90 dBeHL presentation level. • Robust Otoacoustic Emissions as measured by Transient Evoked technology. Emissions eventually disappear by the fourth audiological evaluation (6 months of age)
Normal ABR www.babyhearing.org/
Zachary’s medical history • Born at 33 weeks gestational age • 3 Lb 15 oz • Esophageal atresia type A (a congenital disorder of the digestive system where the esophagus does not fully develop). He was hospitalized for 3 months after birth. Repaired on April 21, 2002. • Jaundice and possible sepsis
Audiological management • 9 months of age: Binaural analog hearing aid which he disliked and did not want to retain longer than his parent’s effort to put them in. • FM system in conjunction with hearing aid did not provide much difference in his functional hearing. • 2 years of age: Changed to binaural digital hearing aids which he loves and uses daily. Significant progress was observed in his speech and his excitement in hearing sounds. He would cup his hand to his ear and sign “what is that?” • Auditory training / aural rehabilitation: once per week until 2 years of age and increased to twice a week after that.
Developmental intervention • 7 months: • Cognitive / Social: • Is more independent (not crying if mom leaves the room for a few minutes). • Explores his environment or objects by reaching for objects and finding hidden objects through locomotion • Gross motor: sits independently, bangs cups together, rakes tiny objects. • Self Help: Is able to finger feed himself, and drink from a cup with adult support. • Communication / speech: • Increases eye contact; communicates his needs through signing, gesturing or verbalizing; responds to environmental sounds and speech by turning his head or vocalizing; and is able to say “mama” and “dada.” • Increases vocalizations
Developmental intervention • 1 year and 18 months: • Cognitive / Social: • Finds objects and is able to play by himself • Points to body part • Increases attention span • Eliminates hand banging and self injurious behavior when frustrated • Gross motor: stands up, holds himself. • Self Help: Feeds himself using utensils, is able to drink from a cup with minimal spillage, is introduced to toilet training. • Communication / speech: • Increases tolerance to hearing aids. • Uses 1 - 3 signs to express his needs, and is able to say “mama” and “dada.” • Increases vocalization • Parents train in communication using ASL and oral language • Increases imitation skills
Developmental intervention • 2 years: • Cognitive / Social: • Masters pre writing skill • Is able to complete puzzles • Recognizes letters and develops pre literacy skills • Gross motor: Jumps forward. • Self Help: Sits at a table during meal, is toilet trained, can eat a variety of foods. • Communication / speech: • Increases accurate production of age appropriate sounds (p, b, m, n, d, t, k, g, w, h, j) • Increases vocabulary • Use 2-3 words phrases spontaneously to request, comment and answer questions • Understands preposition
2 philosophies of how to teach infants and children with auditory neuropathy to communicate • Use of sign language as the child's first language • Use of listening skills and skills in spoken English together with technologies such as hearing aids and cochlear implants • A combination of these two approaches
Aural rehabilitation / auditory training • Age appropriate auditory and communication skills • Wearss hearing aids consistently during his waking hours • Discriminates speech sounds in words, phrases and sentences through audition only • Is able to perform play audiometric testing • Parental partnership and involvement • Understand issues related to auditory neuropathy, options in communication, early literacy skills, deaf mentorship, auditory development, auditory stimulation activities and fostering of oral production. • Increase skills in ASL and become involved in a “shared reading program”
FAMILY CONTRIBUTION • Full active participation in audiological evaluation, management and early intervention • Proficiency in ASL by self study and formal classes • Participation in a deaf mentor pilot project • Careful monitoring of Zachary’s sign and oral language development • Open mindedness to new ideas • Family participation in all of Zachary’s first appointments and Saturday appointments • Creativity in developing new family activities to support Zachary’s needs.
Latest performance • Has a desire to learn; is outgoing, a risk taker, determined, smart, and affectionate; has a great memory and positive behaviors best displayed in a structured environment • Is comfortable with his hearing aids thoughout the day • Uses ASL and spoken language to join 2 or 3 words. • Counts to 5 • Fingerspells a manual alphabet • Is age appropriate for social, motor and self help skills. • Is slightly below his age level for expressive language and mathematical concepts.
FAMILY GOAL ZACHARY TO BE ABLE TO FUNCTION IN SOCIETY AND THE WORK FORCE
Family Belief Children are apt to live up to what you believe of them
Family - Professional Partnership • COMMUNICATION: • Tailored base of learning at home and elsewhere. • Periodic readjustment of management. • Determination of child’s strength and weaknesses. • Creation of and dedication to the same goal: REACHING HIS POTENTIAL
How Hard of Hearing Children Learn to Talkby Nancy Rushmer • They learn to talk through listening with their hearing aids. Because hearing aids do not restore hearing, several adjustments can be used to help them: • Adults should refrain from asking the child to say words. Once a while, it is okay to do that. • Language is caught and not taught. • Children need time to listen and play vocal games. • They need lots of practice with nonsense syllables. • They self correct their own speech. • Children whose attempts to communicate are accepted feels good about himself, tries harder, feels free to “fail” and does learn to talk.
Learning conditions which will be helpful for hard of hearing children: • Wear hearing aids during waking hours • Quiet environment during conversation times • Use lots of descriptive language (talk about what child is looking at, what he is doing and what they both see) • Less directive (except when directing the child to carry out daily routines of eating etc) • Use sign language as a bridge to speech development • Speak clearly • Use lots of repetition (You picked the bird. The bird is blue. Do you like the bird?). • Except child’s speech attempts without correcting them (speech correction is okay by about 4 - 5 years of age, but only when done by a speech therapist or teacher).