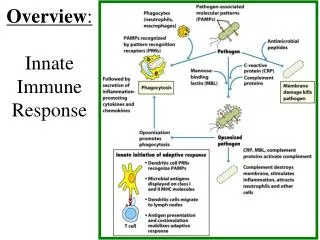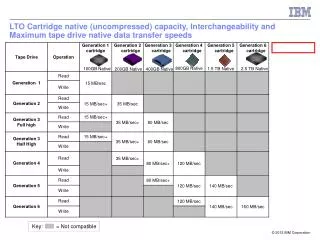
Innate (Native) Immunity in COPD
310 likes | 328 Vues
Innate (Native) Immunity in COPD. Sanjay Sethi MD Professor Pulmonary, Critical Care and Sleep Medicine University at Buffalo, SUNY ssethi@buffalo.edu. COPD: Etiology. Pathogenesis of COPD. NOXIOUS AGENT ( tobacco smoke , pollutants, occupational agent) Airflow Obstruction.

Innate (Native) Immunity in COPD
E N D
Presentation Transcript
Innate (Native) Immunity in COPD Sanjay Sethi MD Professor Pulmonary, Critical Care and Sleep Medicine University at Buffalo, SUNY ssethi@buffalo.edu
Pathogenesis of COPD NOXIOUS AGENT(tobacco smoke, pollutants, occupational agent) Airflow Obstruction Genetic factors Respiratory infection Airway Hyper-reactivity Nutritional factors
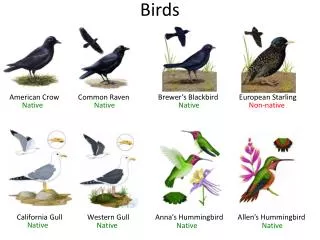
Acute or Chronic Pathogens Typical bacteria Nontypeable Haemophilus influenzae Streptococcus pneumoniae Moraxella catarrhalis Pseudomonas aeruginosa Atypical bacteria Chlamydia pneumoniae Mycoplasma pneumoniae Viruses Influenza Parainfluenza Rhinovirus Adenovirus RSV Fungi Pneumocystis jirvocei Infections in COPD
Acute or Chronic Pathogens Typical bacteria Nontypeable Haemophilus influenzae Streptococcus pneumoniae Moraxella catarrhalis Pseudomonas aeruginosa Atypical bacteria Chlamydia pneumoniae Mycoplasma pneumoniae Viruses Influenza Parainfluenza Rhinovirus Adenovirus RSV Fungi Pneumocystis jirvocei Infections in COPD
Buffalo VA COPD Study Clinic Patient 14 Time Line 1 month ex 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 HI HI HI HI HI HI HI HI HI HI HI HI HI HI HI HI HI HI HI HI HI A A A A B B B B B B C D D D D D D D D D D
38 39 40 42 43 44 45 SDS- PAGE PFGE PCR-P2 gene, sputum pellets Clinic visit 25 30 35 40 45 50 Hi Hi Hi Hi Hi Hi Haemophilus influenzae Murphy et al AJRCCM 2004
Chronic cycle Acute cycle COPD Pathogenesis: Infection Smoking/irritants • Impaired host defenses: • respiratory viruses • new strains of bacteria • environmental irritants Chronic bacterial colonization Impaired lung defense Acute on chronic inflammation (pathogen + host- mediated inflammatory factors) Chronic inflammation (bacterial + host- mediated inflammatory factors) Progressive loss of lung function and deteriorating quality of life
Definition of ‘Colonization’ • Absence of immune response • Absence of damaging effects to the host • Not defined by absence of symptoms Mandell et al, Principles and Practice of Infectious Diseases
Small Airways in COPDInflammatory mucus exudates Hogg et al, NEJM, June 2004
Small Airways in COPDLymphocytes Hogg et al, NEJM, June 2004
Sputum Inflammation and Bacterial Colonization n=27 n=40 n=27 n=40 Banerjee D et al Eur Respir J. 2004 ;23:685-91.
Bronchial Inflammation and Bacterial colonization • Bronchoscopy with BAL • Stable COPD (n = 52) • Healthy Smokers (n = 18) • Non-smokers (n = 8) • PPM colonization • 32% Stable COPD • 42% Smokers • 0% Non-smokers • Increased airway inflammation with bacterial colonization * * Soler et al ERJ 1999;14:1015-22
Bacterial Colonization in Ex-smokers with COPD Sethi et al AJRCCM 2006, 173:991-8
p<0.001 p<0.001 p=0.03 90 80 70 % PMN 60 p=0.02 50 40 p=0.004 30 20 10 0 Ex-smokers Non-smokers COPD PPB+ COPD PPB- Groups Bacterial Colonization in Ex-smokers with COPD p=0.007 p<0.001 p=0.02 450000 400000 350000 PMN/ml 300000 250000 200000 150000 100000 50000 0 COPD PPB+ COPD PPB- Ex-smokers Non-smokers Groups Sethi et al AJRCCM 2006, 173:991-8
p<0.001 p=0.01 p<0.001 p=0.04 p<0.001 1000000 p=0.006 p=0.002 1000 100000 p=0.007 p=0.02 10000 IL-8 pg/ml 100 Active MMP-9 units/ml 1000 100 10 10 1 1 Ex-smokers Non-smokers COPD PPB- COPD PPB+ COPD PPB- COPD PPB+ Ex-smokers Non-smokers Groups Groups Bacterial Colonization in Ex-smokers with COPD Sethi et al AJRCCM 2006, 173:991-8
Chronic cycle Acute cycle COPD Pathogenesis: Infection Smoking/irritants • Impaired host defenses: • respiratory viruses • new strains of bacteria • environmental irritants Chronic bacterial colonization Impaired lung defense Acute on chronic inflammation (pathogen + host- mediated inflammatory factors) Chronic inflammation (bacterial + host- mediated inflammatory factors) Progressive loss of lung function and deteriorating quality of life
Cause or Effect • Discovery of specific pathways of innate immunity • Very small clinically relevant quantities of bacterial molecules are pro-inflammatory • Persistence mechanisms of NTHI not dependent on airway inflammation • Impaired ability of innate defense to clear NTHI • What is the evidence that inflammation induces ‘colonization’ in the lower respiratory tract?
TLR activation and signaling Clin. Sci. (2005) 109, 125-133
NTHI Components are Potent Stimulants of Macrophages • Purified components of NTHI • OMP P6 • OMP P2 • LOS • Total OMP • Biologically relevant concentrations • Sputum levels with 107 bacteria/ml • P6: 4 µg/ml • P2: 95 µg/ml Berenson et al Infect Immun 2005;73: 2728-35
H. influenzae in Bronchial Tissue • NTHI in tissue • 13 of 15 critically ill patients with acute exacerbation • 8 of 24 stable COPD • 0 of 7 healthy controls Bandi et al AJRCCM 2001;164:2114-19
Biofilm Formation by NTHI Jursicek J et al , Infect Immun 2005;73: 3210-8
Chronic cycle Acute cycle COPD Pathogenesis: Infection Smoking/irritants • Impaired host defenses: • respiratory viruses • new strains of bacteria • environmental irritants Chronic bacterial colonization Impaired lung defense Acute on chronic inflammation (pathogen + host- mediated inflammatory factors) Chronic inflammation (bacterial + host- mediated inflammatory factors) Progressive loss of lung function and deteriorating quality of life
Mucociliary clearance Airway antimicrobial peptides Cationic polypeptides Lysozyme Lactoferrin SLPI Cathelicidin Collectins Surfactant protein A Surfactant protein D Defensins Airway epithelium Adherence Cytokine/Chemokine Lung macrophages Opsonophagocytosis Cytokine/Chemokine Inflammatory cells Immunoglobulins IgA Innate Lung Defense Mechanisms
spD ng/ml spA ng/ml Surfactant proteins in COPD SpA SpD 45000 3000 40000 2500 35000 2000 30000 25000 1500 20000 1000 15000 10000 500 5000 0 0 -500 -5000 Non-smokers COPD Ex-smokers Non-smokers COPD Ex-smokers
Cytokine Response of Macrophages to NTHI antigens Berenson C et al AJRCCM 2006
NTHI Strain 14P13H5 * NTHI Strain 14P13H5 2.5 3.5 2 Phagocytosis Index 3 Phagocytosis Index ** 1.5 2.5 * 2 1 ** 1.5 .5 1 0 .5 Non-COPD n = 17 COPD n = 10 Non-smokers n = 9 0 COPD n = 12 Non-COPD n = 17 Non-smokers n = 9 Phagocytosis of NTHI by Lung and Blood Macrophages Alveolar Macrophages Blood Macrophages Berenson C et al JID 2006
Conclusions • Further elucidation of • Mechanisms of colonization and inflammation • Impact of colonization on disease progression • Treatments to interrupt the vicious cycle • Antibiotics (PULSE study) • Alternative treatments that interrupt the inflammatory or infectious process • The British may have been right all the time!!