Download
1 / 27
290 likes | 792 Vues
Rickets of Vitamin D Deficiency The Second Affiliated Hospital of Shantou University Medical College Ma Lian. Review. Rickets : signifying a failure in inernalization of growing bone or osteoid tissue.

E N D
Rickets of Vitamin D DeficiencyThe Second Affiliated Hospital of Shantou University Medical College Ma Lian
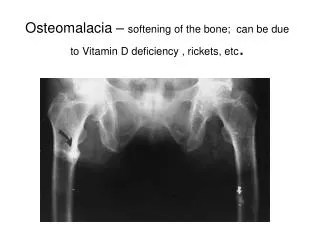
Review Rickets:signifying a failure in inernalization of growing bone or osteoid tissue. Failure of mature bone to mineralize is called osteomalacia.
Etiology • Inadequate direct exposure to ultraviolet rays in sunlight • Inadequate intake of vitD (diet may contain little vitD) • Growth • drug • Disease:hepatic and renal lesions、celiac disease、steatorrhea or cystic fibrosis Or both
About Vitamin-D • Two forms : vitD2 /vitD3 • vitD2 :most as irradiated ergosterol,largely replaced the fish liver oils as source • vitD3 :available in human skin as 7-dehydrocholesterol. • both are hydroxylated in the liver to 25- (OH)2D • in the renal to 1. 25-(OH)2D: facilitate calcium and phosphorus absorpted
Pathology • the epiphyseal plate of metaphysis is well demonstrated. • The cartilage cell is orderly • The calcified matrix forms the epiphyseal plate is regular
The degenerating cartilage, islands of capillaries, osteoblasts, and unmineralized osteoid compose of broad , irregular, rachitic imtermediate zone
Chemical pathology can be conceptualized to be the body’s attempt to maintain normal serum calcium levels. When calcium is lessparathormone is secretedincrease the calcium and phosphorus concentration
Alkaline phosphatase (ALP). (normal level ≦200IU/dL) can be 500UI/dL. But may be normal in infants who have rickets and who are protein or zinc depleted.
aminoaciduria, a decrease of citrate ,and its increased urinary excretion, decreased ability of the kidneys to make an acid urine, phosphaturia, and occasionally ,mellituria. • The parathyroid glands hypertrophy
Clinical manifestations • Early signs: Increased sweating, particularly around the head ,which result in the occipital bone bare
Clinical manifestations • Advanced rickets: • Head: • early signs is craniotabes, • Like a derby hat or ping pong ball .
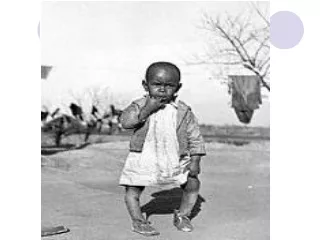
Thorax: rachitic rosary Harrison’s groove Pigen breast deformity children are late in standing and walking
The deformities of the long bones :knobbing and prominence of the epiphyses
Other manifestations: Teeth-erupting may be delayed,the enamel and extensive aries are defected. Muscle tone is poor
Diagnosis • The diagnosis is based on: • a history of inadeuate intake of vitamin D and on clinical observation; • then confirmed chemically ; • by roentgenographic examination .
Differential diagnosis • Scurvy: a ledgelike depression with the chondral or sternal portion is displaced below the osseous ribs. • Chondrodystrophy :irregular、concave outlines of the distal ends of the bones ,no roentgenographic evidence of fraying
Other epiphyseal lesions: congenital epiphyseal dysplasia,cytomegalic inclusion isease ,syphilis ,rubella ,and copper deficiency. • Bowlegs :maybe a familial characteristic. • Vitamin D-resistant rickets and other metabolic disturbances with osseous lesions resembling rickets
Complications • Respiratory infections :bronchitis and bronchopneumonia • pulmonary atelectasis • Anemia due to iron deficiency or accompanying infections
Treatment • Natural and artificial light • oral administration of vitD(preferred) daily administration:vitD3:50-150 µg or 1.25(OH)-D: 0.5-2 µg (except vitD refractory rickets
Administering 15000 µg of vitamin D in a single dose without further therapy for several months may be advantageous. More rapid healing follows, possibly with earlier differential diagnosis from genetic vitamin D-resistant rickets .
Roentgn-ray appearance showing healing • A: active rickets • B: healing after 27 day: new line of calcification • C: after 34 day calcification line dense;periosteal calcification increase • D: complete healing after 3 months
Prognosis • If therapy is given in time , healing begins within a few days and progresses slowly until the normal bony structure is restored • It is not a fatal disease,but complications are more likely to cause death of rachitic children than normal children
Prevention • Can be prevented by exposure to ultraviolet light • Administered vitD :daily requirement of vitamin D is 10µg or 400IU • Vitamin D should also be administered to pregnant and lactating mothers