Download

1 / 21
220 likes | 357 Vues
The Nature of Quality Improvement. Donald M. Berwick, MD, MPP Institute for Healthcare Improvement Testimony to the Secretary’s Advisory Committee on Human Research Protections Washington, DC: March 27, 2008. Aims. Safety Effectiveness Patient-centeredness Timeliness Efficiency Equity.

E N D
The Nature of Quality Improvement Donald M. Berwick, MD, MPP Institute for Healthcare Improvement Testimony to the Secretary’s Advisory Committee on Human Research Protections Washington, DC: March 27, 2008
Aims • Safety • Effectiveness • Patient-centeredness • Timeliness • Efficiency • Equity
IMPROVING SAFETY AT SCALE • 103 ICUs Working on Central Line Infections: • 82% Reduction in Mean Rate • 1,578 Lives Saved • 81,020 Hospital Days Saved • Over $165,000,000 in Costs Averted
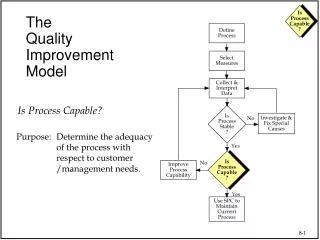
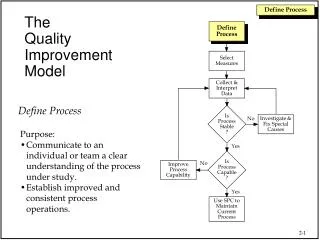
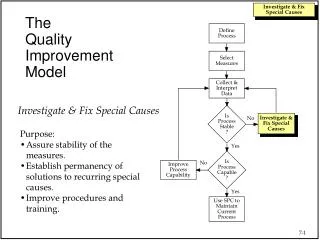
What are we trying to accomplish? How will we know that a change is an improvement? What changes can we make that will result in an improvement? Act Plan Study Do Model for Improvement(Nolan, et al.)
8,015 Donors in 2006 -- Another Recording Breaking Year! -- Collaborative Starts Here
IHS Diabetes Care & Outcomes Audit Mean A1C, 1996-2007 A1C, % year Source: IHS National Diabetes Program Statistics 1996-2007 *p<0.0001 comparing mean A1C levels in FY96 and FY07
Preventing Central Line Infections • Hand hygiene • Maximal barrier precautions • Chlorhexidine skin antisepsis • Appropriate catheter site and administration system care • Daily review of line necessity and prompt removal of unnecessary lines
Central Line Associated Bloodstream Infections (CLABs)(from Rick Shannon, MD, West Penn Allegheny Health System)
The Campaign “Planks” -- Six Changes That Save Lives • Deployment of Rapid Response Teams • Delivery of Reliable, Evidence-Based Care for Acute Myocardial Infarction • Medication Reconciliation • Prevention of Central Line Infections • Prevention of Surgical Site Infections • Prevention of Ventilator-Associated Pneumonias
Six Additional Planks • Prevent Pressure Ulcers • Reduce Methicillin-Resistant Staphylococcus Aureus (MRSA) Infection • Prevent Harm from High-Alert Medications • Reduce Surgical Complications (the Surgical Care Improvement Project (SCIP)) • Deliver Reliable, Evidence-Based Care for Congestive Heart Failure • Get Boards on Board
Rapid Response Results: Benedictine Hospital 43% Reduction
“Informed Consent…” NOTICE TO OUR PATIENTS This hospital – our leaders, Board, and staff …. □does □does not make continual, informed changes in its processes of care, based on current and new science, to improve safety, effectiveness, patient-centeredness, timeliness, efficiency, and equity, for you. We continually measure our results and compare them to those of others. Our results over time are displayed below….
Conclusions • “Quality improvement” is primarily a component of proper management, not the creation of new knowledge from research. • Unlike researchers, clinicians and health care organizations have an obligation to improve patient care quality. • Ethical management requires continual improvement, ethically managed, but that is not a human subjects research issue.
What Could OHRP Do? • Clarify that QI work was not meant to come under IRB jurisdiction under the Common Rule. • Encourage health care leaders and clinicians to set standards and articulate guidelines for the ethical conduct of QI, but as a matter separate from “human subjects research.” • Clarify that neither measurement nor learning nor comparison groups nor publication make a QI project “human subjects research.”