Download

1 / 24
240 likes | 478 Vues
Evidence for adjuvant radiation therapy benefiting breast cancer patients with 1 to 3 positive lymph nodes treated with a modified radical mastectomy and systemic therapy.

E N D
Evidence for adjuvant radiation therapy benefiting breast cancer patients with 1 to 3 positive lymph nodes treated with a modified radical mastectomy and systemic therapy Shaheenah Dawood, Ana M. Gonzalez-Angulo, Wendy Woodward, Funda Meric-Bernstam, Kelly Hunt, Aman U. Buzdar,Gabriel N. Hortobagyi, Thomas A. Buchholz The University of Texas M. D. Anderson Cancer Center Departments of Breast Medical Oncology, Surgical Oncology and Radiation Oncology Dubai Hospital, U.A.E, Department of Medical Oncology Departments of Breast Medical Oncology, and Quantitative Sciences (Abstract number :507
Disclosure • I have no relevant relationships to disclose.
Postmastectomy RadiationOxford: Mastectomy +/- XRT Trials Breast Recurrence Breast Ca Deaths LN - Disease • Local Recurrence • 2/3 reduction • Breast Ca Survival • none in LN- • 5% for LN+ 8% vs. 3% 28% vs. 31% LN + Disease 60%vs. 55% 29% vs. 8%
There is current consensus that postmastectomy radiation therapy is indicated for patients whose tumors are either > 5cm and/or >= 4 positive lymph nodes. • Whether adjuvant radiation therapy should be used for patients with early stage breast cancer with tumors < 5cm and up to 3 positive axillary lymph nodes treated with mastectomy and systemic therapy is controversial.
Aim • Thus the purpose of this retrospective study was to determine if adjuvant radiation therapy had an impact on survival for patients with early stage breast cancer with up to 3 positive axillary lymph nodes treated with surgery and systemic therapy
Methodology Stage I and II Breast Cancer Mastectomy + no Radiation Segmental Resection + Radiation
Methodology • Database : M.D Anderson Breast Cancer Management Systems Database • Inclusion criteria : • Female patients • Diagnosed between 1980 and 2007 • Surgery • T1/T2 N0 or T1/T2/N1 • Tumors <5 cm • Nodes <4 • Exclusion criteria : • Male patients • More than one primary • Hormone receptor positive who did not receive hormone treatment • Mastectomy and radiation therapy • Segmental resection and no radiation
Outcome Measures • Follow-up cut-off was 30th December 2008. • Outcome measures: • Local-Regional Disease Free Survival (LRDFS): Calculated from the date of diagnosis to the date of first locoregional metastases or last follow-up. • Distant Disease Free Survival (DDFS): Calculated from the date of diagnosis to the date of first distant metastases or last follow-up.
Statistical Analysis • Kaplan-Meier method used to calculate outcome and segmental resection with radiation patients were compared to those with mastectomy without radiation using two-sided log rank tests. • Cox proportional hazards was used adjusting for differences in patient and tumor characteristics between the two groups.
Multivariate Analysis of LRDFS • Models adjusted for age, grade, hormone receptor status, HER2 status, • menopausal status, race, neoadjuvant chemo, anthracycline use, taxane use, • and lymphovascular invasion
LRDFS Among LN Negative Groups T1N0 (N=1191) T2N0 (N=997) 5- Year Estimates Segmental : 92% Mastectomy: 91% P=0.93 5- Year Estimates Segmental : 91% Mastectomy: 89% P=0.99
LRDFS Among LN Positive Groups T1N1 (N=876) T1N2 (N=676) 5- Year Estimates Segmental : 91% Mastectomy: 90% P=0.65 5- Year Estimates Segmental : 91% Mastectomy: 87% P=0.009
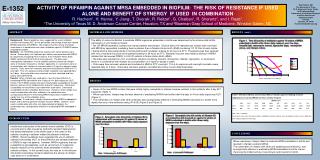
Adjusted Hazard Ratios for LRDFS among various subgroups Forrest Plot For Sub-Groups Favors Mastectomy Favors Segmental Whole Cohort T1N0 T1N0 T2N0 T2N0 T1N1 T1N1 T2N1 T2N1 No Neoadjuvant group (HR = 2.62 , 95% CI 1.26-5.46, P =0.00099 Hazard Ratios LDFS
Multivariate Analysis for DDFS • Models adjusted for age, grade, hormone receptor status, HER2 status, • menopausal status, race, neoadjuvant chemo, anthracycline use, taxane use, • and lymphovascular invasion
DDFS Among LN Negative Groups T1N0 (N=1191) T2N0 (N=997) 5- Year Estimates Segmental : 87% Mastectomy: 86% P=0.11 5- Year Estimates Segmental : 85% Mastectomy: 80% P=0.38
DDFS Among LN Positive Groups T1N1(N=876) T2N1(N=676) 5- Year Estimates Segmental : 90% Mastectomy: 85% P=0.004 5- Year Estimates Segmental : 77% Mastectomy: 68% P=0.0177
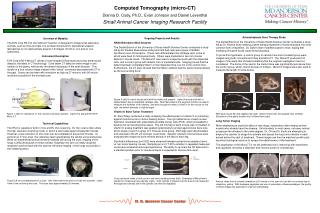
Adjusted Hazard Ratios for DDFS among various subgroups Favors Mastectomy Favors Segmental T1N0 T2N0 T1N1 HR = 1.71 , 95% CI 1.15-2.52, P =0.007 T2N1 No Neoadjuvant group (HR = 1.54, 95% CI 0.98-2.23, P =0.061)
Conclusions • Patients with tumors <5 cm and 1 to 3 positive lymph have an increase risk of loco-regional and distant disease recurrence when radiation is not used as a component of their local-regional treatment. • The benefit of radiation appears to be most pronounced for patients with T2N1 disease with the benefit still unclear for those with T1N1 disease.
Limitations • We acknowledge the following limitations: • Retrospective nature of the study • Comparing women who underwent segmental resection with radiation to a comparable cohort who underwent mastectomy to assess the benefit of post mastectomy radiation may not be ideal. • However the results of our study are hypothesis generating and will need to be confirmed in prospective randomized clinical trials.
Acknowledgement Mentors Dr. Thomas A. Buchholz Dr. Ana M. Gonzalez-Angulo Dr. Mona Al Rhukhaimi Dr. Farid Khalifa