Comprehensive Overview of Mandibular Fractures: Anatomical Considerations and Treatment Strategies
350 likes | 598 Vues
This detailed guide explores the various types, classifications, and management principles of mandibular fractures, including anatomical considerations, clinical assessment, radiographic techniques, and surgical interventions. Learn about the principles of treatment, definitive management strategies, and surgical complications associated with mandibular fractures.

Comprehensive Overview of Mandibular Fractures: Anatomical Considerations and Treatment Strategies
E N D
Presentation Transcript
Mandibular fracture is more common than middle third fracture (anatomical factor) It could be observed either alone or in combination with other facial fractures Minor mandibular fracture may be associated with head injury owing to the cranio-mandibular articulation Mandibular fracture may compromise the patency of the airway in particular with loss of consciousness 2
Mandible was more sensitive to lateral impact than frontal one Frontal impact is substantially cushioned by opening and retrusion of the jaw Fracture of condyle regarded as a safety mechanism to the patient Long canine tooth and partially erupted wisdoms represent line of relatively weakness 3
Anatomical considerations Attached muscles: Masseter Temporalis Medial and lateral pterygoid Mylohyoid Geniohyoid and genioglosus anterior belly of digastrics 4
Anterior Muscles • Weaker force • Mylohyoid, geniohyoid, genioglossus, platysma, anterior digastric muscles • Muscle action depresses and retracts (open mandible)
Posterior Muscles: • Stronger force • Temporalis Muscle • Masseter Muscle • Medial Pterygoid Muscles • Lateral Pterygoid Muscles
Sites of fractures Condyle fracture Intracapsular fracture Extracapsular fracture High condyle neck fracture Low condylar fracture Angle/ ramus fracture (body fracture) Canine region (parasymphesial fracture) Midline fracture (symphesis fracture) Coronoid fracture (rare) 7
Classification by Favorability • Favorable • Unfavorable
Classification by Type of Fracture • Open versus Closed • Fracture Pattern: Communited, oblique, transverse, greenstick • Pathologic: fractures secondary to bone disease (eg, osteogenic tumors, osteoporosis)
Dental Classification • Class I • Class II • Class III
Clinical assessment and diagnosis History of trauma (traumatized patients with possible head injury) and facial injuries Clinical Examination ▶ Extra oral Inspection (assessment of asymmetery, swelling, ecchymosis, laceration and cut wounds) Palpation for eliction of tenderness, pain, step deformity and malfunction ▶ Intra oral bleeding, heamatoma, gingival tear, disturbance of occlussion and step deformity and sensory and motor deficiency 14
Tongue blade test • Tongue blade test: have patient bite down while you twist. If no fracture, you will be able to break the blade.
Radiographs Plain radiograph OPG Lateral oblique PA mandible AP mandible (reverse Townes) Lower occlusal CT scan 3-D CT imaging 16
Principles of treatmentsimilar to elsewhere fractures in the body Reduction of fragments in good position Immobilization until bony union occurs These are achieved by: Close reduction and immobilization Open reduction and rigid fixation Other objective of mandible fracture treatment: Control of bleeding Control of infection 18
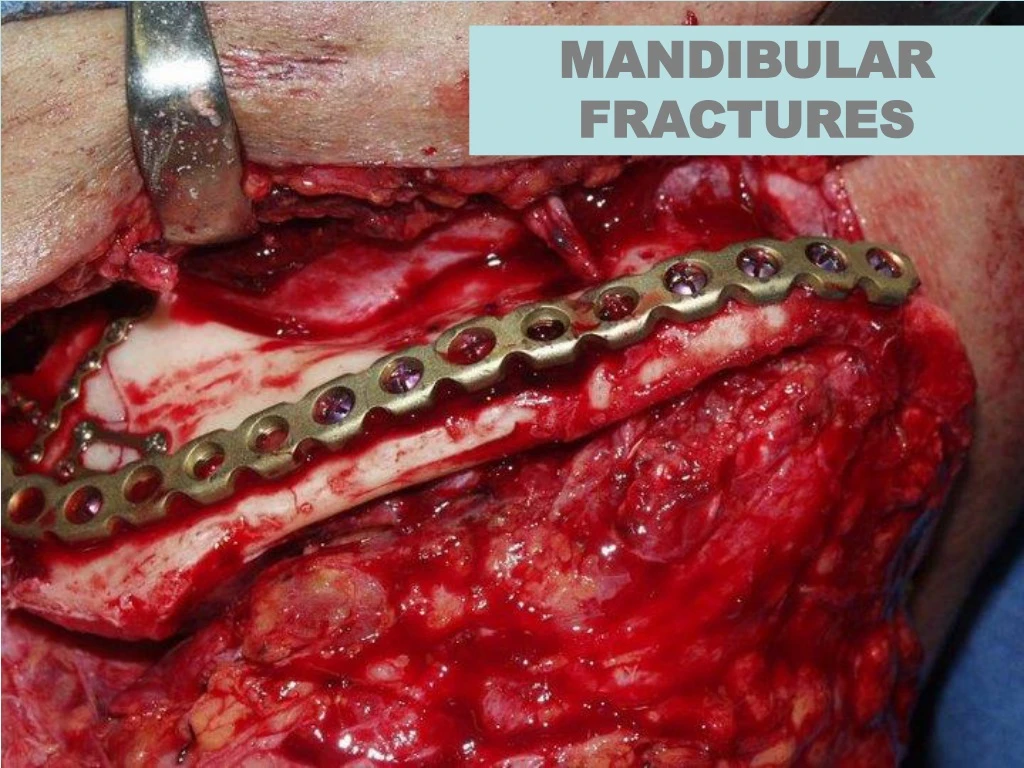
Definitive treatment Soft tissue repair Debridment Irrigation with saline and antibiotics Closure in layers Dressing Reduction and fixation of the jaw ▶Close reduction and IMF (traditional method by means of manipulation) ▶Open reduction and semi-rigid fixation (using inter-ossous wirings) ▶Open reduction and rigid fixation (using bone palates osteosynthesis) 19
Close reduction Bonded brackets IMF screws Dental wiring: Direct wiring Eyelet wiring Local anesthesia orsedation Minimal displacement IMF for 6 weeks Treatment can be performed under GA or LA and when surgery is contraindicated 20
Close reduction Arch bars ▶IMF prior to rigid fixation ▶For the purpose of close reduction 21
Gunning’s splint Old modality Edentulous patient Rigid fixation is not possible To establish the occlusion 22
Open reduction and fixation Intraoral approach Extraoral approach ▶ Submandibular approach 23
Rigid fixation Intraossous wiring Plates and screws Kirchener wire Lag screws 24
Reconstruction palate Severe trauma Loss of part of the bone 25
Condylar fractures Intraoral approach Ramus incision Extraoral approach Preauricular approach Retromandibular approach 26
Fracture mandible in children Close reduction Open reduction and fixation Plating at the inferior border Resorbable plates 27
Teeth in the fracture line The fracture is compound into the mouth The tooth may be damaged or lose its blood supply The tooth may be affected by some preexisting pathology 28
Management of teeth retained in fracture line Good quality intra-oral periapical radiograph Insinuation of appropriate systemic antibiotic therapy Splinting of tooth if mobile Endodontic therapy if pulp is exposed Immediate extraction if fracture becomes infected Follow up for 1 year and endodontic therapy if there is a loss of vitality 29
Absolute indications Longitudinal fracture Dislocation or subluxation from socket Presence of periapical infection Infected fracture line Acute pericoronitis Relative indications Functional tooth that would be removed Advanced caries or periodontal diseases Tooth in untreated fracture presenting more than 3 days after injury 30
Surgical Complications • Chin and Lip Hypesthesis • Osteomyelitis • Malunion • Nonunion • Plate Exposure • Marginal Mandibular Nerve Injury • Necrosis of Condylar Head (Aseptic Necrosis) • TMJ Ankylosis • Dental Injury