Physiological optics. Ophthalmologic tools.
Physiological optics. Ophthalmologic tools.

Physiological optics. Ophthalmologic tools.
E N D
Presentation Transcript
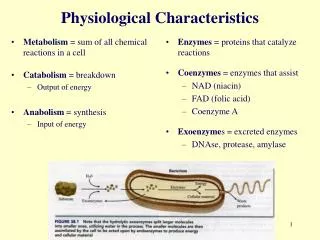
Eye is like a camera. The external object is seen like the camera takes the picture of any object. Light enters the eye through a small hole called the pupil and is focused on the retina, which is like a camera film. Eye also has a focusing lens, which focuses images from different distances on the retina. The colored ring of the eye, the iris, controls the amount of light entering the eye. It closes when light is bright and opens when light is dim.
Cornea • Front part of the eye, transparent. Protects front of eye and bends light to form an image on the retina. • Pupil • A black hole in the center of the iris. Allows light to enter into the eye. • Iris • Pigmented (the color of the eyes). Its muscles contract and relax to alter the size of its central hole or pupil. Protects the photoreceptors in the retina from being damaged by too much light. • Retina • The lining at the back of the eye containing two types of photoreceptor cells. It is a screen on which images are formed as a result of light being focused onto it by the cornea and lens. • Lens • Transparent, flexible disc behind the iris attached by muscles. Brings the light entering through the pupil to a focus on the retina. • Macula • The macula contains a high concentration of photoreceptor cells that convert light into nerve signals. Send visual signals to the brain. • Optic nerve • Bundle of sensory neurons at back of eye. Carries signals from the photoreceptors of the retina to the brain.
The Eye as an Optical System • The eye can be considered as an optical system with a positive power of about 58 D. It has two main refractive elements, the cornea and the lens. The cornea bulges in the front of the eyeball, and because its first surface is in contact with air, it bears most of the power of the eye (about 45 D). The eyeball has a mean length of 24 mm, and the image is formed at the interior of the back side, where the retina is found. The aqueous humor, which has a refractive index of 1.336, is located in the midst of the cornea and the lens. The volume behind the lens is filled with vitreous humor, with index 1.337. The power of the lens is not fixed, and it can expand surface curvature and power via the ciliar muscles surrounding it. This process is called accommodation, and serves to bring near objects into focus.
Ammetropies and Refractive Error • Emmetropia is defined as the condition for which the relaxed eye (without accommodation) images a distant object onto the retina (fovea). • We say that the eye suffers from refractive error when it fails to bring into focus the image of a distance object. The condition in which a refractive error occurs is called ammetropia.
Myopia: The image of a distant object forms before the retina because the eye is too powerful, too large, or both. Refractive error is negative and the remote point is located in front of the eye. Near point is also located in front of the eye, at a smaller distance from it. Glasses or contact lenses with concave lenses will correct the eye's error and bring the images of far-off objects into sharp focus on the retina. Concave lenses curve inward, like the inside of a bowl.
Hyperopia: The image of the distant object forms behind the retina as a result of any of the followingreasons: 1) the eye does not attain enough power, 2) the eye is too small, or 3) combination of both. In case the refractive error is smaller than the amplitude of accommodation, the hyperopic eye may bring the images of distance objects into focus via accommodation. The remote point of the hyperopic eye is located behind (to the right of) the same. The near point can be located at the right of the remote, when amplitude of accommodation is smaller than the refractive error. Otherwise, it is located at a finite distance in front of the eye. When blurred vision occurs, an ophthalmologist may prescribe glasses or contact lenses, with convex lenses to reinforce focusing power. A convex lens is rounded outward, like the outer surface of a globe.
Astigmatism: The eye shows different powers at different meridian planes. We will assume that the meridian planes with maximum and minimum power are orthogonal (regular astigmatism). These are called the principal meridians. The power difference between them is termed the astigmatism of the eye. When characterizing astigmatism, aside from the value of the difference between powers, it is also necessary to provide the orientation of any of the principal meridians. The condition can be treated with cylindrical lens glasses or with hard contact lenses. A special "toric" soft lens is also available now. Cylindrical lenses are shaped like slices from a tube and compensate for the defects of the eye by bending the light rays inward.
Presbyopia: The amplitude of accommodation reduces with age and along with it, the ability to focus near objects. When amplitude of accommodation reduces be- low 3 D (which usually happens between 40 and 50 years of age in Europe), comfortable reading at 33 cm is no longer possible, and ophthalmic compensation is necessary for activities using near vision. This is a common condition and simple convex lens reading glasses are used to correct it.
LENSES • Materials used in spectacle lens Spectacle lenses are made from three different sources of materials. In spectacle lens, there are many materials used. Natural media, quartz (or) rock crystal, semi-precious stones (i.e. Topaz, Ruby, etc) were widely used for making lenses.
Glass materials • Now-a-days spectacle lenses are made from either plastic or a high quality glass material. Although many types of glass materials are used in optical industry, crown glass (1.523) material is extensively used for making single vision ophthalmic lenses. It is a soda-lime-silica material that contains about 70% silica, • 12% calcium oxide and 15% sodium oxide and some other materials in smaller percentages like potassium, borax, arsenic etc. Flint glass, material (1.620) is used in the making of bifocal or achromatic lens. It contains 60%, lead oxide, 30% silica, 8% soda and potash and small percentage of arsenic.
Plastic materials • Plastic lenses are generally made from two different materials. They are: • 1. Original plastic lens made of (PMMA) Polymethylmethocrylate • 2. Modern hard resin lens from allyl diglycol carbonate (CR 39) which is harder and more resistant to scratches than other plastic lens materials. • Plastic lenses are made from a very high quality material as glass. Plastic lenses are about half the weight of glass and are highly impact-resistant.
Corrective lens • Multi focals designs • There are two basic types of multifocal lenses used. • 1. In one-piece (or) solid type designs, the same material (glass or plastic) is used throughout the lens and changing the curvature of lens varies the power. (Fig.1) • The Executive bifocal (glass or plastic) is a modern version of the original Benjamin Franklin bifocal which has two lenses in each eye of which the lower half is used for closer view and the upper half for distance.
2. The fused multifocal lenses are made of two or more glass materials with different refractive indexes when the segment with higher indices is fused into the main lens; the surfaces of fused lens have no change of curvature. • (Fig. 2) Falling into a category between one piece and fused lenses are cement bifocals. Two lenses of the same type having the same index of refraction are attached together to form a lens with the special features of the one-piece lens.
Progressive addition lens • Among the various types of multifocal designs progressive addition lens has become very popular now-a-days. Over 150 PAL designs have been introduced since 1984 with more than 70 PAL designs currently available in the market. • The progressive addition lenses gradually increases in power as the line of sight comes downwards through the lens.
High power lenses • In high-powered lenses a strong distortions would occur through the edges of the lens inherently. To avoid these distortions special lens have been designed to minimize the distortion and the weight of these lenses. • The types most commonly used are • (i) Lenticular lens • (ii) Aspheric lens
Lenticular lens • The lenticular lens may be described as a small in diameter or circular and mounted on a longer diameter, thin planocarrier which is edged to fit into the frame. The main disadvantage of lenticular lens is that it gives a bull’s eye effect making it more conspicuous than the other lens.
Aspheric lens • An Aspheric lens is particularly designed to eliminate the “pincushion” distortion in the (aphakia) high plus lenses.
Fresnel lenses • Fresnel lenses are sheets of Polyvinyl chloride, and it was designed by Augustine Fresnel. The Fresnel lenses are used for various purposes. It is used in ships and lighthouses as a “light-condensing lens”. As Fresnel lens is thin and weightless it would make an ideal cataract lens but it shows a pattern of fine concentric circles, which gives poor cosmetic appearance to the wearers.
Safety lens • The risk of damage to the eye from broken glasses is minimized by the use of safety glass. It is however advisable to use it for those who are engaged in industrial works and sports.
Plastic hard-resin lenses • These are safety lenses with no additional treatment, because they will take abuse much greater than that required to shatter a standard glass lens. A shattered hard-resin lens does not have the sharp splinters typical for broken glass. Hard resin lenses are superior to hardened glass for welding for if not metal may splatter on the lens. • Another type of safety lens is the laminated lens in which a sheet of plastic is sandwiched between two pieces of glasses. If the lens is shattered, the glass particles adhere to the plastic.
Polycarbonate lens • First introduced in plano safety goggles in industry, polycarbonate lenses are one the most impact-resistant lenses now available in the market. In this regard they out perform plastic and glass heat-treated or chemically treated and thus easy to scratches. • Polycarbonate is now being moulded into ophthalmic Rx lenses that are coated to substantially reduce their tendency to scratch.
A contact lens (also known simply as a contact) is a corrective, cosmetic, or therapeutic lens usually placed on the cornea of the eye. Leonardo da Vinci is credited with describing and sketching the first ideas for contact lenses in 1508, but it was more than 300 years later before contact lenses were actually fabricated and worn on the eye. Rigid ones were produced and marketed first. Modern soft contact lenses were invented by the Czech chemist Otto Wichterle and his assistant Drahoslav Lím, who also invented the first gel used for their production.
Corrective contact lenses • A corrective contact lens is designed to improve vision. For many people, there is a mismatch between the refractive power of the eye and the length of the eye, leading to a refraction error. A contact lens neutralizes this mismatch and allows for correct focusing of light onto the retina. Conditions correctable with contact lenses include myopia (near or short sightedness), hypermetropia (far or long sightedness), astigmatism and presbyopia.
Cosmetic contact lenses • A woman wearing a cosmetic type of contact lenses; the enlarged section of the image shows the grain produced during the manufacturing process. As the lines of printed dots are curved, these lenses were manufactured by printing onto a flat sheet and then shaping the sheet.
Therapeutic contact lenses • Soft lenses are often used in the treatment and management of non-refractive disorders of the eye. A bandage contact lens protects an injured or diseased cornea from the constant rubbing of blinking eyelids thereby allowing it to heal. They are used in the treatment of conditions including bullous keratopathy, dry eyes, corneal ulcers and erosion, keratitis, corneal edema, descemetocele, corneal ectasis, Mooren's ulcer, anterior corneal dystrophy, and neurotrophic keratoconjunctivitis. Contact lenses that deliver drugs to the eye have also been developed.
Types of Contact Lenses Daily-wear soft lenses (Yearly) • The most popular type of lenses. • Made of soft, flexible plastics that allow oxygen to pass through to the eyes. • Short period of adaptation. • More comfortable and more difficult to dislodge than RGP lenses. • Available in bifocals and colors. • Ideal for active and sportive lifestyles. • Lens Care Products are very simple to use.
Types of Contact Lenses Daily disposable soft lenses • No lens Care products are required. • Clean, fresh and sterile lenses replaced every day. • Ideal for active lifestyles. Monthly disposable soft lenses • Clean, fresh and sterile lenses when replaced every month. • Available in most prescriptions. • Useful as spare lenses.
Types of Contact Lenses • Gas Permeable (GP) • Made of harder plastic materials that do not contain water. • Made of slightly flexible plastics, not as flexible as soft contacts, but they allow more oxygen to pass through to the eyes than do soft lenses. • Comfortable for most people after a short period of adaptation • Sharper vision than with soft contact lenses • Causes less infection than soft lenses. • Relatively long life (3-4) years • Available in bifocals or multifocals • Daily-wear and extended-wear designs available • Disadvantage: • They may slip off the center of the eye more easily • Once you don't wear these lenses for about week, it needs an adaptation period before they're comfortable again.
Types of Contact Lenses • Ortho-K • A vision correction therapy for patients with moderate myopia and low amounts of astigmatism. • It involves wearing a contact lens retainer while you sleep to gently and painlessly corrects the surface of your eye. • This process is reversible and non-surgical. • Daytime free of contact lenses and spectacles. • Ideal for sports, swimming and for dusty or dirty environments.
Torch lightDescription and purpose: A torch light is the first instrument an ophthalmologist uses to examine the eye of a patient. A good torch light should give a circular patch of light of nearly uniform brightness.
OphthalmoscopeDescription and Purpose: Ophthalmoscopes are of two kinds direct and indirect. Direct Ophthalmoscope which is usually referred to as ophthalmoscope, and sometimes briefly as the ‘scope’, is a very handy instrument for the examination of the retina around the fundus. Light from a bulb is reflected at right angles and projected as a spot through the iris of the patient to illuminate the retina. This reflection is achieved using a front silvered mirror or partially silvered mirror or a total reflecting prism in different scopes. The illuminated retina is seen directly by the doctor through the iris of the patient. A disc with lenses of different powers is provided in the instrument and a lens of required power can be brought in the line of sight to correct any refractive error of the patient or of the doctor himself if he does not look through his spectacles. The doctor looks just above the front silvered mirror and the reflecting prism or through the partially silvered reflector mentioned earlier. An image magnified nearly fifteen times is seen.
RetinoscopeDescription and purpose: Different types of retinoscope are used. One of them, the streak retinoscope described here, is the most common instrument. It is used in the objective evaluation of the power of the spectacles needed to correct the refractive error of patients and also in determining the axis and cylindrical power needed for patients with astigmatism. As in direct ophthalmoscope (chapter-5) light from a bulb is reflected at right angles and is projected on to the eye of the patient. The light is either a rectangular patch (known as plane mirror mode) or a streak of light of variable width (concave mirror mode). The instrument is generally used in the cubicle of refractionist/optometrist which is usually dark.
Indirect Ophthalmoscope • Description and Purpose: The modern Indirect Ophthalmoscope functions as the eye piece of a stereomicroscope for which a hand held high positive aspheric lens (17D, 20D or 30D) serves as the objective. When viewed properly, a magnified image of the retina is seen. Some of the advantages of the instrument as compared to the direct ophthalmoscope are (1) stereoscopic view (2) greater field of view (3) increased illumination and (4) reduced distortion. An additional advantage is that the doctor is at a distance from the patient. However, the final image seen is inverted and the magnification is much lesser than in a direct ophthalmoscope.