Download
1 / 38
380 likes | 514 Vues
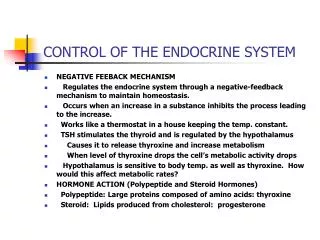
Endocrine Control of Growth and Metabolism. 23. About this Chapter. Adrenal glucocorticoids Thyroid hormones Growth hormone Tissue and bone growth Calcium balance. Adrenal Glucocorticoids. Structure and function of the adrenal gland. Figure 23-1a. Cortisol.

E N D
About this Chapter • Adrenal glucocorticoids • Thyroid hormones • Growth hormone • Tissue and bone growth • Calcium balance
Adrenal Glucocorticoids Structure and function of the adrenal gland Figure 23-1a
Cortisol The HPA pathway for the control of cortisol secretion CRH- Corticotrophic Releasing Hormone ACTH- Adrenocorticotrophic hormone Cortisol- lipophilic hormone that enters the nucleus and althers gene expression, transcription, and translation Figure 23-3
Cortisol Cortisol receptors are found in every tissue in the body and release varies throughout the day.
Cortisol • Promotes gluconeogenesis- stimulates the liver to increase blood glucose levels • Causes breakdown of skeletal muscle proteins – releases amino acids to act as substrates for gluconeogenesis • Enhances lipolysis- releases glycerol for gluconeogenesis and fatty acids for cellular respiration • Suppresses the immune system- reduces inflammation and other immune system functions. When used as a medication (ibuprofen) it need to be taper off once not needed. • Causes negative calcium balance - reduces absorption and increases bone matrix breakdown • Influences brain function – affect mood, memory, and learning.
Cortisol: Therapeutic Drug • Suppresses the immune system – prevents cytokine & antibody production, helps prevent organ rejection, • Inhibits the inflammatory response – reduced the mobility of leukocytes • Used to treat: • Bee stings, poison ivy, and pollen allergies • Prevents rejection of transplanted organs
Hypercortisolism • Adrenal tumor that autonomously secretes cortisol- primary hypercortisolism • Pituitary tumor that autonomously secretes ACTH (adrenocorticotropic hormone)- secondary hypercortisolism • Cushing’s disease- hyperglycemia, muscle breakdown, lipolysis, extra fat in trunk and face, • Iatrogenic hypercortisolism- resulting from cortisol therapy (exogenous cause) Individual with Cushing’s Syndrome cause by adrenal or pituitary tumor Figure 23-5
Hypocortisolism • Less common than Cushing’s syndrome • Addison’s disease- hereditary defects in enzymes needed to make the steroid hormones • Hyposecretion of all adrenal steroid hormones • Autoimmune destruction of adrenal cortex
CRH Family • CRH (corticotropin-releasing hormone) – is involved in the following: • Inflammation and immune response • Decreases food intake • Signals that mark onset of labor • Linked to anxiety, depression, and other mood disorders • Urocortin: brain neuropeptide related to CRH
ACTH and Melanocortins • ACTH- secretion stimulated by CRH • Synthesized from POMC (pro-opiomelanocortin) • POMC products include -endorphin- an opiate that blocks pain • Processed in tissue outside the pituitary- produces different molecules • Additional processing creates -MSH- it inhibits food intake in brain and acts on melanocytes in skin • Melanocortins • Family name for the MSH (melanocyte-stimulating hormone) hormones and ACTH **there are five melanocortin receptors in the adrenal gland and skin cells (melanocytes)
Thyroid: Structure Figure 23-7a
Thyroid Thyroid hormones are made from iodine and tyrosine-they are thermogenic so they increase O2 for oxydative phosphorylation. Thyroid hormones synthesis takes place in the colloid of the thyroid follicle Figure 23-8
Pathway of Thyroid Hormone Control Negative feedback mediated by thyroid hormones reaches the hypothalamus to stop production at the pituitary. In thyroid disorders negative feedback is removed Figure 23-12
Hyperthyroidism • Affects: metabolism, the nervous system, & the heart • Increases oxygen consumption and metabolic heat production – patients have a high metabolism and since they generate a lot of heat they don’t tolerate hot environments well. • Increase protein catabolism and may cause muscle weakness – the body breaks down the protein in muscle cells which also causes weight loss. • Hyperexcitable reflexes and psychological disturbances – may affect the nervous tissue structure and receptors. • Influence -adrenergic receptors in the heart - increases heart rate and contraction force
Thyroid Exophthalmus, caused by hypertrophy of tissues in the eye socket, is a sign of hyperthyroidism Figure 23-15
Hypothyroidism • Slow metabolic rate and oxygen consumption – less tolerant to cold because they don’t generate much internal heat due to lower metabolic rate. • Decreases protein synthesis – causing brittle nails, thinning hair, dry thin skin, and myxedema. In children it retards growth. • Slowed reflexes, slow speech and thought processes, and feelings of fatigue – nervous response is slower or less efficient • Cretinism in infants- decreased mental capacity • Bradycardia – slower heart rate
Thyroid A man with goiter due to excessive TSH stimulation –immunoglobulins released in hyperthyroidism mimic TSH and stimulate thyroid enlargement (Grave’s Disease) may also be caused by excess thyroid-stimulation in hypothyroidism Figure 23-13
Thyroid Goiter can occur in both hyperthyroidism and hypothyroidism Figure 23-14a
Normal Growth • Growth hormone and other hormones - GH, thyroid hormones, insulin, and sex hormones at puberty are important for normal growth and development. • An adequate diet – sufficient calories, protein, vitamins and minerals provide the building blocks for proper growth. • Absence of stress – stressful environments cause children to release cortisol which stunts growth • Genetics – height potential is inherited
Pathway of Growth Hormone Control Growth hormone promotes anabolism of proteins. It is released by anterior pituitary and IGF provides negative feedback cycles. GH is bound to a binding protein to keep it from being excreted in urine and to increase its lifetime. Figure 23-16
Growth Hormone In adults, pulses of GH are released during the first two hours of sleep. The greatest amount of GH release occurs during puberty.
Growth Hormone • Severe GH deficiency leads to dwarfism • Oversecretion of GH in children leads to giantism • Oversecretion of GH in adults leads to acromegaly
Tissue and Bone Growth • Growth is determined by increase in soft tissue (weight) and bone length (height) • Tissue growth requires hormones and paracrines • GH and IGFs required for protein and cell division for hypertrophy and hyperplasia • Thyroid hormone plays permissive role- directly affects nervous system development • Insulin supports tissue growth- stimulates protein synthesis and provides energy, has a permissive role • Bone growth requires adequate dietary calcium • Hydroxyapatite- most common form of calcium **review parts of a long bone as covered in anatomy
Bone Growth Compact and trabecular bone Bone length increases at the epiphyseal plate and diameter with matrix deposits around surface Figure 23-18
Bone growth Epiphysis is the end of a long bone. Diaphysis is the shaft of a long bone. Bone gr owth Compact bone Dividing chondrocytes add length to bone. Epiphyseal plate is the site of bone growth. Chondrocyte Direction of growth Chondrocytes produce cartilage. Old chondrocytes disintegrate. Cartilage Osteoblasts lay down bone on top of cartilage. Diaphysis Newly calcified bone Osteoblast Linear growth of long bones takes place at the epiphyseal plates- sex hormones eventually inactivate epilhyseal plates. Figure 23-19
Calcium • Important signal molecule – increased Ca 2+ concentrations allows for cell responses like exocytosis and muscle contraction. Active transport is needed to decrease cytosolic Ca 2+ concentration. • Part of intercellular cement that holds cells together at tight junction – integrated component of the cell junction protein structure • Cofactor in the coagulation cascade – The body will always have enough calcium to mediate coagulation • Affects the excitability of neurons – hypocalcemia causes the NS to become hyperexcitable, thus increasing muscle contraction. Hypercalcemia cause NS to be hypoexcitable causing depressed neuromuscular activity.
Calcium Balance in the Body ECF [Ca2+] 2.5 mM Electrochemical gradient Active transport Cells [free Ca2+] 0.001 mM KEY PTH = parathyroid hormone Calcium in the ECF is either bound to proteins or free to diffuse. Calcium in ICF is stored in mitochondria, or ER, or free in cytosol Figure 23-20 (2 of 5)
Calcium Balance in the Body ECF Bone Calcitonin [Ca2+] Ca2+ 2.5 mM PTH Calcitriol Cortisol Electrochemical gradient Active transport Cells [free Ca2+] 0.001 mM KEY PTH = parathyroid hormone Bone is largest calcium reservoir. It is stored as hydroxyapartite crystals. Calcium is released to maintain plasma levels Figure 23-20 (3 of 5)
Calcium Balance in the Body Small intestine Dietary calcium Ca2+ Calcitrol (PTH, prolactin) ECF Bone Calcitonin [Ca2+] Ca2+ 2.5 mM PTH Calcitriol Cortisol Electrochemical gradient Active transport Cells [free Ca2+] 0.001 mM KEY PTH = parathyroid hormone Only 1/3 of the calcium ingested is absorbed. Absorption is regulated by a hormone. A healthy diet needs to be high in calcium in order to match the amount excreted Figure 23-20 (4 of 5)
Calcium Balance in the Body Small intestine Dietary calcium Calcium in feces Ca2+ Calcitrol (PTH, prolactin) Some calcium is secreted into the small intestine. ECF Bone Kidney Passive filtration Calcitonin [Ca2+] Ca2+ in kidney tubules Ca2+ 2.5 mM PTH PTH Calcitriol Calcitonin Cortisol Electrochemical gradient Active transport Cells [free Ca2+] 0.001 mM KEY Ca2+ in urine PTH = parathyroid hormone Total body calcium = intake output Calcium is mostly excreted by the kidneys through urine and a small amount is lost in feces. Calcium reabsorption at the kidneys is regulated by hormones or transport proteins Figure 23-20 (5 of 5)
Calcium Balance Osteoclasts are responsible for bone resorption – a low pH environment and proteases are needed to dissolve bone matrix. Figure 23-21
Calcium Balance • Parathyroid hormone: increases plasma Ca. concentration by stimulating its release/reabsorption from bone, kidney, and intestine. • Mobilizes calcium from bone- does not bind osteoclast but promotes release of paracrines the increse its activity • Enhances renal reabsorption- prevents excessive build up of calcium in urine • Indirectly increases intestinal absorption- used calcitrol to increase absorption • Calcitriol – vitamin D3, most important in adults, acts bone, liver, intestine • Calcitonin- targets osteoclasts and reduces bone resorption, thus dropping blood ]Ca 2+ ]
Calcium Balance: Parathyroid Glands Figure 23-22
Endocrine Control of Calcium Balance Figure 23-23
Calcium Balance • Calcium and phosphate homeostasis are linked- most phosphate in the body is found in bone, it is processed similarly in the same three organs that process calcium by the same hormones. • Phosphate is key ingredient of hydroxyapatite • Phosphate has other roles • Energy transfer and storage • Activation and deactivation of enzymes, transports, and ion channels • Part of DNA and RNA backbone
Osteoporosis Normal bone (left) and bone loss in osteoporosis (right) Figure 23-24