Download
1 / 40
410 likes | 738 Vues
Hormonal Control of Nutrient Metabolism and Storage. Dr. Mujeeb Ahmed Shaikh Assistant Professor AlMaarefa College. Learning Objectives. Describe the effect of insulin on glucose, fat, and protein metabolism.

E N D
Hormonal Control of Nutrient Metabolism and Storage Dr. Mujeeb Ahmed Shaikh Assistant Professor AlMaarefa College
Learning Objectives • Describe the effect of insulin on glucose, fat, and protein metabolism. • Explain what is meant by counter-regulatory hormones, and describe the actions of glucagon, amylin, somatostatin, gut-derived hormones, epinephrine, growth hormone, and the adrenal cortical hormones in the regulation of blood glucose levels.
Nutrient Metabolism and Storage • The body uses glucose, fatty acids, and other substrates as fuel to satisfy its energy needs.
Glucose Metabolism and Storage • The brain and nervous system rely almost exclusively on glucose as a fuel source. • Other tissue can use fatty acids & ketone bodies • Body tissues obtain glucose from the blood. • In normal person the fasting blood glucose levels are tightly regulated between 80 and 90 mg/dL (4.4 and5.0 mmol/L).
After meal 2/3 of the glucose is removed from the blood & stored in liver as glycogen. • Between meals, the liver releases glucose as a means of maintaining the blood glucose within its normal range. • Extra glucose - glycogen / fats. • After muscle & liver get saturated the extra glucose used for FA & triglyceride synthesis.
Between meals, the liver releases glucose as a means of maintaining the blood glucose within its normal range. • The liver synthesizes glucose from amino acids, glycerol, and lactic acid in a process called gluconeogenesis.
Glucose Regulating Hormones • The hormonal control of blood glucose resides largely within the endocrine pancreas. • The pancreas is made up of two major tissue types: the acini and the islets of Langerhans. • Acini – digestive juices into duodenum • islets of Langerhans - secrete hormones into the blood.
Islet cells • Alpha cells – Glucagon • Beta cells – insulin & amylin • Delta cells - Somatostatin. • PP cells - pancreatic polypeptide
Endocrine pancreas: Islets of Langerhans Alpha Beta cells Delta cells PP cells cells Insulin Pancreatic Glucagon Somatostatin and amylin polypeptide
Functions of Pancreatic Hormones • Glucagon: causes cells to release stored food into the blood • Insulin: allows cells to take up glucose from the blood • Amylin: slows glucose absorption in small intestine; suppresses glucagon secretion • Somatostatin: decreases GI activity; suppresses glucagon and insulin secretion
Anabolism and Catabolism available foodstuffs stored foodstuffs Anabolism (in blood) (in cells) Insulin, anabolic steroids glucose glycogen Catabolism amino acids proteins glucagon, epinephrine, free fatty acids triglycerides cortisol liver can convert amino acids and free fatty acids into ketones
Insulin and Glucagon Are the Main Controls Anabolism available foodstuffs stored foodstuffs Insulin (in blood) (in cells) , anabolic steroids glucose glycogen Catabolism amino acids proteins Glucagon , epinephrine, free fatty acids triglycerides cortisol liver can convert amino acids and free fatty acids into ketones
Insulin • Insulin is the only hormone known to have a direct effect in lowering blood glucose levels. • The actions of insulin are threefold: • it promotes glucose uptake by target cells and provides for glucose storage as glycogen, • it prevents fat and glycogen breakdown, and • It inhibits gluconeogenesis and increases protein synthesis • Insulin acts to promote • fat storage by increasing the transport of glucose into fat cells • It also facilitates triglyceride synthesis from glucose in cells and inhibits the intracellular breakdown of stored triglycerides.
Insulin also inhibits protein break-down and increases protein synthesis by increasing the active transport of amino acids into body cells, and it inhibits gluconeogenesis, or the building of glucose from new sources, mainly amino acids.
Glycogen Glucose-P Protein Pyruvate Free fatty acids CO2 Ketoacids Liver Metabolic Effects of Insulin Glucose Glucose Amino acids Adipose tissue Muscle Plasma Stimulate Glucose Free fatty acids Ketoacids Amino acids Inhibit
Approximate Rates of Insulin Secretion at Different Blood Glucose Levels 100% Insulin Response ( ) 50% 0 40 80 120 160 200 240 Plasma glucose (mg/dl)
The C-peptide chains can be measured clinically, and this measurement can be used to study beta cell function (i.e., persons with type 2diabetes with very little or no remaining beta cell function will have very low or nonexistent levels of C-peptide in their blood, and thus will likely need insulin replacement for treatment).
Secretion of insulin occurs in a pulsatile fashion. After exposure to glucose, which is a nutrient secretagogue, a First-phase release of stored preformed insulin occurs, followed by a second-phase release of newly synthesized insulin. • Serum insulin levels begin to rise within minutes after a meal, reach a peak in approximately 3 to 5 minutes, and then return to baseline levels within 2 to 3 hours. • Insulin has a half-life of approximately 15 minutes once it is released into the general circulation.
Factors Affecting Insulin Secretion Inhibitors Stimulators Glucose Mannose Galactose Amino acids Arginine Lysine Leucine Alanine Free fatty acids, Ketoacids Glucagon (direct and indirect effects) Gastro intestinal hormones Glucagon like peptide 1 (GLP-1) Glucose dependantInsulinotropic Peptide (GIP) Secretin Fasting Exercise Somatostatin Neural influences Sympathetic activity- -adrenergic stimulation norepinephrine, epinephrine) Neural influences Vagal activity (acetylcholine) b-adrenergic stimulation Drugs like Sulfonylurea
Processing of Proinsulin and C-Peptide Connecting peptide HOOC NH2 20 1 S S 1 15 5 A-chain 10 S B-chain 30 S S S 5 25 Proinsulin 10 20 15 C-Peptide S S 20 COOH NH2 1 5 10 15 S Insulin S A-chain S S COOH NH2 30 10 15 20 25 1 5 B-chain
Cell membranes are impermeable to glucose, they require a special carrier, called a glucose transporter, to move glucose from the blood into the cell. • GLUT 1, GLUT 2, GLUT 3, GLUT 4. • GLUT-4 is the insulin-dependent glucose transporter for skeletal muscle and adipose tissue
GLUT-2 is the major transporter of glucose into beta cells and liver cells. It has a low affinity for glucose and acts as a transporter only when plasma glucose levels are relatively high, such as after a meal. • GLUT-1 is present in all tissues. It does not require the actions of insulin and is important in transport of glucose into cells of the nervous system.
Glucagon • A polypeptide molecule produced by the alpha cells of the islets of Langerhans, maintains blood glucose between meals and during periods of fasting. • Glucagon produces an increase in blood glucose. • Initiate breakdown of glycogen between meals • Gluconeogenesis • Makes fatty acids available for use as energy
Factors Affecting Glucagon Secretion Inhibition Stimulation Hypoglycemia Amino acids Arginine Alanine Gastrointestinal hormones Cholecystokinin (CCK) Gastrin Fasting Exercise Neural influences Vagal activity-acetylcholine Sympathetic activity- -adrenergic stimulation (norepinephrine, epinephrine) Glucose Somatostatin Insulin (direct effect) Gastrointestinal hormones Secretin Glucagon-like peptide-1 (GLP-1) Free fatty acids Ketoacids Neural influences a-adrenergic stimulation
Approximate Rates of Insulin & Glucagon Secretion at Different Blood Glucose Levels 100% 100% Insulin Response ( ) Glucagon Response ( ) 50% 50% 0 0 40 80 120 160 200 240 Plasma glucose (mg/dl)
Amylin, Somatostatin, and Gut-Derived Hormones • A polypeptide that is co secreted with insulin from the beta cells. • Plasma levels of amylin increase in response to nutritional stimuli to produce inhibition of gastric emptying and glucagon secretion. • he less soluble and insoluble forms, which may cause degeneration of the beta cells and contribute to the pathogenesis of overt diabetes
Somatostatin • Its a polypeptide hormone containing only 14 amino acids that has an extremely short half-life. • Secreted by the delta cells acts locally in the islets of Langerhans to inhibit the release of insulin and glucagon. • It also decreases gastrointestinal activity after ingestion of food. • Almost all factors related to ingestion of food stimulate somatostatin secretion.
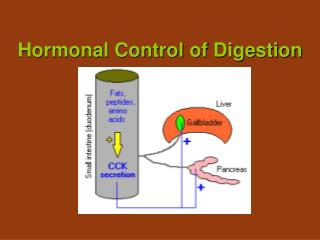
Incretins • Several gut derived hormones have been identified as having what is termed an incretineffect, meaning that they increase insulin release after an oral nutrient load. • The two hormones that account for about 90% of the incretin effect are glucagon like peptide-1, which is released from L cells in the distal small bowel, and glucose-dependent insulinotropic polypeptide, which is released by K cells in the upper gut (mainly the jejunum).
Counter regulatory Hormones • They counteract the storage functions of insulin in regulating blood glucose levels during periods of fasting, exercise, and other situations that either limit glucose intake or deplete glucose stores. • The catecholamines, • Growth hormone, and • Glucocorticoids.
Epinephrine • helps to maintain blood glucose levels during periods of stress. • Glycogenolysis in the liver • Inhibits insulin release • Increasing the breakdown of muscle glycogen stores. • A direct lipolytic effect on adipose cells,
Growth Hormone • Increases protein synthesis • Mobilizes fatty acids from adipose tissue, and antagonizes the effects of insulin. • Chronic hypersecretion of growth hormone, as occurs in acromegaly, can lead to glucose intolerance and the development of diabetes mellitus.
Glucocorticoid Hormones • Gluconeogenesis by the liver • Hypoglycemia is a potent stimulus for cortisol secretion. • In predisposed persons, the prolonged elevation of glucocorticoid hormones can lead to hyperglycemia and the development of diabetes mellitus.
Hormonal Interactions in the Maintenance of Blood Glucose Concentration Glucose Production (Liver Hepatic Glucose Output) (-) (+) (+) Glucagon Epinephrine Glucocorticoids Growth Hormone Blood Glucose Insulin (+) (-) Glucose Consumption (Skeletal Muscle and Adipose Tissue)
_ _ + + Hormonal Effects on FFA Production in Adipose Tissue Epinephrine Insulin Triglycerides Fatty Acids Insulin Hormone Sensitive Lipase glucose -Glycerol-P Growth hormone Cortisol Epinephrine glycerol FFA