Download

1 / 28
280 likes | 451 Vues
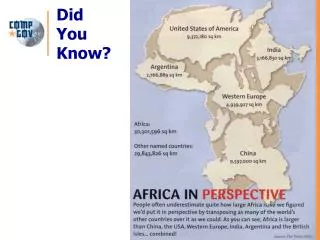
Prescription of Medicines in Nigeria… Abuse and Implications for the Health of Nigerians. Catherine Olufunke Falade Professor of Pharmacology & Therapeutics, UI and Consultant Clinical Pharmacologist, UCH, Ibadan, Nigeria. What are Medicines?.

E N D
Prescription of Medicines in Nigeria… Abuse and Implications for the Health of Nigerians Catherine Olufunke Falade Professor of Pharmacology & Therapeutics, UI and Consultant Clinical Pharmacologist, UCH, Ibadan, Nigeria
What are Medicines? • The word medicine is derived from the Latinarsmedicina, meaning the art of healing. • Medicineor medication, can be loosely defined as any chemical substance intended for use in the medical diagnosis, cure, treatment or prevention of disease • Medicines used from mediaeval times were derived from herbs
Statue of Asclepius, the Greek god of medicine, holding the symbolic Rod of Asclepius with its coiled serpent
Medicines - Classification • Medicines into two main classes • Prescription medicines and • Over-the-counter medicines. • Dangerous, powerful, or habit-forming medicines to be used under a health care provider's supervision can be sold only by prescription. • The prescription must be written by a physician, dentist, or advanced practice nurse; otherwise the pharmacist is forbidden to prepare and fill it.
Prescription • An order for medication, therapy, or therapeutic device given by a properly authorized person, which ultimately goes to a person properly authorized to dispense or perform the order. • A prescription is usually in written form; can be emailed from a secure encrypted computer system, written, phoned, or faxed; • It includes • The patient's name (± address), • The date, the ℞ symbol (superscription), • The medication prescribed (inscription), • Directions to the pharmacist or other dispenser (subscription), • The acceptability of dispensing a generic, • Directions to the patient that must appear on the label, • Prescriber's signature, and, • Inn some instances an identifying number.
Prescription- Historical perspectives • Early medicines made up of multiple ingredients requiring complex preparation • Latin was as the standard language of prescription to ensure understanding between physicians and pharmacists and consistency in pharmaceutical composition. • The symbol Rx = abbreviation for reciperethe Latin word for “take” or “take thus” as a direction to a pharmacist preceding the physician’s “recipe” for preparing a medication. • Prescription no longer written in Latin but a lot abbreviations have been preserved in prescription writing
Parts of a Prescription • There are four parts to a drug prescription. • The SUPERSCRIPTION, the symbol ℞ from the Latin recipe, meaning “take.” • The INSCRIPTION,specifying the ingredients and their quantities. • The SUBSCRIPTION, which tells the pharmacist how to compound the medicine. • The SIGNATURE; it is usually preceded by an S to represent the Latin signa, meaning “mark.” The signature is where the health care provider indicates what instructions are to be put on the outside of the package to tell the patient when and how to take the medicine and in what quantities. The pharmacist keeps a file of all the prescriptions filled.
Prescription -Abbreviations • How Often to Take Your Medicationad lib - freely, as neededbid - twice a dayprn - as neededq - everyq3h - every 3 hoursq4h - every 4 hoursqd - every dayqid - four times a dayqod - every other daytid - three times a day • When to Take Your Medicationac - before mealshs/nocte- at bedtimeint - between mealspc - after meals • How Much Medication to Takecaps - capsulegtt - dropsmg - milligramsml - millilitersss - one halftabs - tabletstbsp - tablespoon (15ml)tsp - teaspoon (5ml) • How to Use Your Medicationad - right earal - left earod - right eyeos - left eyeou - both eyespo - by mouths or ø - withoutsl - sublingualtop - apply topically
Why prescription writing? • Clinical training for undergraduate students often focuses on diagnostic rather than therapeutic skills. Sometimes students are only expected to copy the prescribing behavior of their clinical teachers, or existing standard treatment guidelines, without explanation as to why certain treatments are chosen. • Although pharmacological knowledge is acquired, practical prescribing skills remain weak. • In one study, medical graduates chose an inappropriate or doubtful drug in about half of the cases, wrote one-third of prescriptions incorrectly, and in two thirds of cases failed to give the patient important information. • So good training is needed before poor habits get a chance to develop.
Dangers of bad Prescription habits • Bad prescribing habits lead to ineffective and unsafe treatment, exacerbation or prolongation of illness, distress and harm to the patient and higher costs. • They also make the prescriber vulnerable to influences which can cause irrational prescribing e.g. • Patient pressure, • Bad example of colleagues and • High powered salesmanship. • Later on, new graduates will copy them, completing the circle.
The Process of Rational Prescribing Step 1: Define the patient's problem Step 2: Specify the therapeutic objective Step 3: Verify whether your P-treatment is suitable for this patient Step 4: Start the treatment Step 5: Give information, instructions and warnings Step 6: Monitor (stop) the treatment
Step 6: Monitoring the treatment • If the patient does not return, he is probably better. • If there is no improvement and he does come back there are three possible reasons: • The treatment was not effective; • The treatment was not safe, e.g. because of unacceptable side effects; or • The treatment was not convenient, e.g. the dosage schedule was hard to follow or the taste of the tablets was unpleasant. • Combinations are also possible.
Steps in choosing a P-drug • Define the diagnosis • Specify the therapeutic objective • Make an inventory of effective groups of drugs • Choose an effective group according to criteria • Choose a P-drug
Irrational use of medicines • More than 50% of all medicines are prescribed, dispensed or sold inappropriately, and half of all patients fail to take medicines correctly. • The overuse, underuse or misuse of medicines harms people and wastes resources. • More than 50% of all countries do not implement basic policies to promote rational use of medicines. • In developing countries, less than 40% of patients in the public sector and 30% in the private sector are treated according to clinical guidelines. • A combination of health-care provider education and supervision, consumer education, and an adequate medicines supply is effective in improving the use of medicines, while any of these interventions alone has limited impact.
What is rational use of medicines • Rational use of medicines refers to the • Correct, proper and appropriate use of medicines. • Rational use requires that patients receive • the appropriate medicine, • in the proper dose, • for an adequate period of time, and • at the lowest cost to them and their community
Incorrect use of Medicines • WHO estimates that more than half of all medicines are prescribed, dispensed or sold inappropriately, and that half of all patients fail to take them correctly. • This incorrect use may take the form of overuse, underuse and misuse of prescription or non-prescription medicines • Common problems include: • Polypharmacy(use of too many medicines); • Overuse of antibiotics and injections; • Failure to prescribe in accordance with clinical guidelines; • Inappropriate self-medication
Incorrect use of Medicines -2 • In Nigeria and other developing countries: • Less than 40% of patients in the public sector and 30% in the private sector are treated according to clinical guidelines for common diseases • Less than 60% of children with acute diarrhoea receive necessary oral rehydration therapy yet more than 40% receive unnecessary antibiotics • Only 50% of people with malaria receive the recommended first-line antimalarial • Only 50–70% of people with pneumonia are treated with appropriate antibiotics, yet up to 60% of people with viral upper respiratory tract infection receive antibiotics inappropriately
Consequences of Incorrect use of Medicines • Antimicrobial resistance. • Resistance prolongs illnesses and hospital stays, and can even cause death, leading to very high costs (US$ 4–5 billion per year in the United States of America and €9 billion per year in Europe) • Adverse drug reactions and medication errors. • Harmful reactions to medicines caused by wrong use, or • Allergic reactions to medicines can lead to increased illness, suffering and death. • Adverse drug reactions have been estimated to cost millions of dollars each year
Consequences of incorrect use of medicines - 2 • Lost resources. • Between 10–40% of national health budgets are spent on medicines. • Out-of-pocket purchases of medicines can cause severe financial hardship to individuals and their families. • If medicines are not prescribed and used properly, billions of dollars of public and personal funds are wasted. • Eroded patient confidence. • Exacerbated by the overuse of limited medicines, drugs may be often out of stock or at unaffordable prices and as result erode patient confidence. • Poor or negative health outcomes due to inappropriate use of medicines may also reduce confidence.
What factors contribute to incorrect use of medicines? • Lack of skills and knowledge. • Lack of prescriber knowledge of optimal diagnostic approaches, • Lack of independent information such as clinical guidelines, • Lack of opportunity for patient follow-up, or fear of possible litigation, lead to improper prescription and dispensing of medicines. • Inappropriate unethical promotion of medicines by pharmaceutical companies. • Most prescribers get medicine information from pharmaceutical companies rather than independent sources such as clinical guidelines. This can often lead to overuse. Some countries allow direct-to-consumer advertising of prescription medicines, which may lead to patients pressuring doctors for unnecessary medicines. • Profits from selling medicines. • Drug retailers prescribe and sell medicines over-the-counter. • The more they sell the more income they generate, leading to overuse of medicines, particularly the more expensive medicines. • Unrestricted availability of medicines. • In Nigeria, prescription medicines such as antibiotics, are freely available over-the-counter. This leads to overuse, inappropriate self-medication and non-adherence to dosing regimes.
Factors that contribute to incorrect use of medicines contd. • Overworked health personnel. • Prescribers have too little time with each patient, ± → to poor diagnosis and treatment. • Prescribers rely on prescribing habit as they do not have the time to update their knowledge of medicines. • Unaffordable medicines. • People may not purchase medicine at all or buy incomplete course of treatment • Instead they may seek alternatives, such as medicines of non-assured quality from the Internet or other sources, or medicines prescribed to family or friends. • Lack of coordinated national pharmaceutical policy. • Less than half of all countries implement the basic policies recommended by WHO to ensure the appropriate use of medicines. • These include appropriate measures and infrastructure for monitoring and regulation of medicines use, and training and supervision for prescribing health workers.
What can be done to improve rational use of medicines? WHO Recommendations • Countries should implement national programmes to promote rational use of medicines through policies, structures, information and education. These include: • A national body to coordinate policies on medicine use and monitor their impact; • Evidence-based clinical guidelines for training, supervision and supporting decision-making about medicines; • Lists of essential medicines used for medicine procurement and insurance reimbursement; • Drug (medicines) and therapeutics committees in districts and hospitals to monitor and implement interventions to improve the use of medicines; • Problem-based training in pharmacotherapy and prescribing in undergraduate curricula; • Continuing medical education as a requirement of licensure;
What can be done to improve rational use of medicines? WHO Recommendations • Publicly available independent and unbiased information about medicines for health personnel and consumers; • Public education about medicines; • Elimination of financial incentives that lead to improper prescribing, such as prescribers selling medicines for profit to supplement their income; • Regulations to ensure that promotional activities meet ethical criteria; and • Adequate funding to ensure availability of medicines and health personnel. • The most effective approach to improving medicines use in primary care in developing countries is a combination of education and supervision of health personnel, consumer education, and ensuring an adequate supply of appropriate medicines. Any of these alone have limited impact.
WHO Response To improve rational medicine use, WHO: • Monitors global medicines use and pharmaceutical policy • Provides policy guidance and support to countries to monitor medicines use and to develop, implement and evaluate national strategies to promote rational use of medicines • Develops and delivers training programmes to national health professionals on how to monitor and improve medicines use at all levels of the health system.
Case studies - 1 • The poor anti-asthma prescribing behaviour among these doctors is associated with a low level of participation at update training on asthma management and poor awareness of asthma guidelines. The Nigerian Medical Association and the Nigerian Thoracic Society should urgently address these problems. Fawibe et al 2012 • The pattern of prescription drug use in Nigerian Army hospitals is unsatisfactory. It is characterised by high number of drugs per prescription, high rate of antibiotic usage and unscientific prescription by doctors. There is a need for further education and research on rational drug use among prescribers in Nigerian military health facilities. Adebayo & Hussain2010 • Antihypertensive utilization in Ilorin, Nigeria like some parts of the country conforms to the guidelines for the management of hypertension in blacks with majority of patients on diuretics particularly in combination with other agents. Angiotensin converting enzyme inhibitors are increasingly being used whereas beta-blockers and angiotensin receptor antagonists are still less utilized. Olanrewaju et al 2010
Case studies - 2 • Benefits of antihypertensive combination therapy, and demonstrate an apparent higher efficacy of calcium channel blocker monotherapy than diuretic monotherapy in blood pressure lowering in the study population. Major limitations of this work include its retrospective nature and the inability to determine the actual patients' adherence to therapy. Etuk et al 2008 • Polypharmacy exists in all the hospitals. The average number of drugs per encounter for the majority of the hospitals was above 4. Less than half of the prescriptions had the correct dose of chloroquine. This study can serve as a baseline for intervention on irrational prescribing. Ainaet al 2009 • Unlicensed and off-label medicines are widely used for children in the centres studied. Further research on this subject is recommended in other parts of Nigeria and Africa. Okechukwu & Agomo2012
Case studies -3 • Prescription practices are far from ideal, and continuing education, as well as development of prescription practice guidelines is suggested. Government intervention and change in clinician attitudes may be needed to improve use of newer medications. Adeponle et al 2008 on Psychotropic drugs prescription at two regional psychiatric hospitals in northern Nigeria. • This initial report suggests that Nigerian dentists are not well informed about the potential interaction between antibiotics and combined oral contraceptive and the extra precautions to be taken when antibiotics is prescribed for women on COC pills. A cross-section of Nigerian dentists prescribed antibiotics 1-3 times during a normal week. Arigbedeet al 2008 • The pattern of antimalarial drugs prescription in the study center in most cases did not meet the recommended guidelines. The prescriptions were predominantly chloroquine, instead of artemisinin based. The death rate was comparatively high. Measures to raise the level of awareness among the practitioners on the current National policy on malaria treatment through seminars and workshops were suggested. Etuk et al 2008
Thank you for listening!!!