Hepatitis E
Hepatitis E . Dr. Sachin Verma MD (Medicine), FICM, FCCS Consultant Internal Medicine & Critical Care Ivy Hospital Mohali – 71. Hepatitis E virus: An important pathogen in tropical and subtropical regions. Type of Hepatitis. A. B. C. D. E. Source of. feces. blood/. blood/.

Hepatitis E
E N D
Presentation Transcript
Hepatitis E Dr. SachinVerma MD (Medicine), FICM, FCCS Consultant Internal Medicine & Critical Care Ivy Hospital Mohali – 71
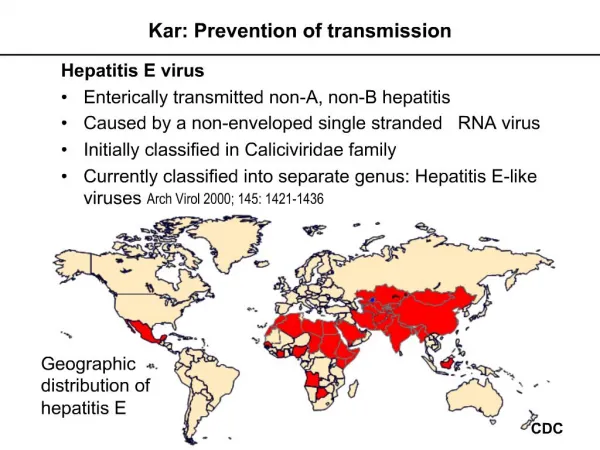
Hepatitis E virus: An important pathogen in tropical and subtropical regions
Type of Hepatitis A B C D E Source of feces blood/ blood/ blood/ feces virus blood-derived blood-derived blood-derived body fluids body fluids body fluids Route of fecal-oral percutaneous percutaneous percutaneous fecal-oral transmission permucosal permucosal permucosal Chronic no yes yes yes no infection Prevention pre/post- pre/post- blood donor pre/post- ensure safe exposure exposure screening; exposure drinking immunization immunization risk behavior immunization; water modification risk behavior modification
Introduction • 1978: epidemic of icteric viral hepatitis in the Kashmir Valley involving 52000 cases with 1650 fulminant forms and 1560 deaths. • 1980: MS Khuroo suggested that this epidemic of hepatitis might have been caused by new virus .(Am J Med 68:818-23,1980).
1983 : Balayan demonstrated that this virus, at difference of non-A non-B virus, is transmitted by fecal-oral route. (Intervirology 20:23-31,1983). • 1991 : By transmitting the disease to monkeys the virus was recovered and its morphology and genome were identified
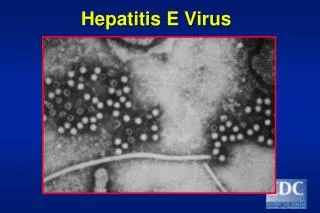
Structure of hepatitis e virus • icosahedral and nonenveloped • Diameter of approximately 34 nanometers • Single strand of RNA approximately 7.5 kilobases in length.
Classified as the single member of the genus herpesvirus in the family Herpesviridae • Three large opening reading frames (ORFs) of the positive-sense RNA of HEV have been described
Phylogenetic analysis • Four genotypes • Upto 24 subtypes .
Epidemiology of Hepatitis E • Central and South-East Asia, North and West Africa, and in Mexico • Common in hot climate area • sporadic cases of hepatitis E - south-east and central Asia, the Middle East, northern and western Africa, and North America
Major outbreaks • Kashmir: 52,000 cases in 1978 • Kanpur :79,000 cases in 1991 • China :100,000 cases between 1986 and 1988
Recent outbreaks • 2004 : Chad , 1,442 reported cases and 46 deaths. • 2004: Sudan , 6,861 cases and 87 deaths. • 2011: minor outbreak reported in Tangail, Bangladesh. • June,2012 : an outbreak was reported in Ichalkaranji, Maharashtra.3232 cases and 18 deaths and 3 died in Shiroltaluka of Kolhapur Maharashtra
Mode of Transmission • Spread • faecal-oral route • Food and waterborne disease • Ingestion of raw or uncooked shellfish has been the source of sporadic cases in endemic areas • Risk factor • poor sanitation
Can we call hepatitis e an emerging zoonotic infection ??? • HEV strains have been genetically identified including domestic and wild pigs, chickens, deer, rabbits, mongeese, dogs, cats, sheep, goats, rodents, cattle, and non-human primates,
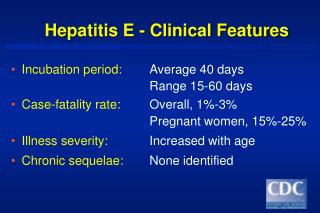
Hepatitis E - Clinical Features • Incubation period:Average 40 days • Range 15-60 days • Case-fatality rate: Overall, 1%-3%Pregnant women, 15%-25% • Illness severity: Increased with age • Chronic sequelae: ????
Classic presentation:Infectious Hepatitis • Phase 1 - Viral replication; Patients are asymptomatic during this phase. • Phase 2 – Prodromal • Phase 3 - Icteric phase • Phase 4 - Convalescent phase; symptoms and icterus resolve. Liver enzymes return to normal. • Severe cases may cause fulminant hepatitis
Hepatitis E and chronicity…… • Reports of presence of HEV RNA and chronic hepatitis in liver and kidney transplant recipients • Total counts of lymphocytes and of CD2, CD3, and CD4 T cells were significantly lower in patients in whom chronic disease developed.* • *Kamar N, Selves J, Mansuy JM, Ouezzani L, Péron JM, Guitard J, Cointault O, Esposito L, Abravanel F, Danjoux M, Durand D, Vinel JP, Izopet J, Rostaing L.N Engl J Med. 2008 Feb
Kamar N, Selves J, Mansuy JM, Ouezzani L, Péron JM, Guitard J, Cointault O, Esposito L, Abravanel F, Danjoux M, Durand D, Vinel JP, Izopet J, Rostaing L.N Engl J Med. 2008 Feb
Higher fatalities in pregnant women • Case fatality rate is 20%, and this rate increases during the second and third trimesters. • Reported causes of death include encephalopathy , disseminated intravascular coagulation and fulminant hepatic failure
Liver transplant patients at risk • HEV infection can lead to chronic hepatitis. • If the patient has antibodies against HEV, the risk of reactivation is extremely low
HEV has emerged as the leading identified cause of autochthonous acute hepatitis among adults • Colson P, MoalV, MotteA, et al.,EASL 2011; abstract A-343
Incidence of HEV infection in Solid organ transplantation: • ≥1% after liver transplantation in the Netherlands and in France[Haagsmaetal.,2009;Kamaretal.,2008] • 4.5% in kidney transplant recipients in France [Kamaretal.,2008]. • 0.4-3.4 % in liver transplant recipients in the Netherlands, Germany and Spain [Haagsmaetal.,2009;Pischkeetal.,2010;Butietal.,2010].
Furthermore,in these previous studies, progression toward chronicity occurred in about 60% of kidney-transplant recipients infected with HEV.
HEV and HIV The Rate of Anti-HEV seropositivity increased with the progression of HIV infection, reaching 43.3% in AIDS patients and 38.1% in those who died from AIDS.
The percentages of HBcAb, HBsAg, anti-HCV and anti – HEV (58.5, 14.5, 58.5 and 6.6% respectively) were significantly higher in HIV-positive patients than in control groups.
Diagnosis of hepatitis E • Hepatitis E should be suspected in outbreaks of waterborne hepatitis occurring in: • Developing countries, • Especially if the disease is more severe in pregnant women, • Or if hepatitis A has been excluded • If laboratory tests are not available, epidemiologic evidence can help in establishing a diagnosis
Acute hepatitis E is diagnosed when the presence of IgM anti-HEV is detected • Storage of serum samples is acceptable for several days at 4°C • Anti-HEV will be preserved at – 20°C,
HEV RNA can be detected in acute phase in serum or faeces by PCR in approximately 50% of cases. Can be detected 2 wks before and 2 wks after the onset of symptoms • Immune electron microscopy is positive in only about 10% of cases
To confirm the results of EIA or ELISA tests, • Western blot assays to detect IgM and IgG anti-HEV in serum can be used
Are Anti-HEV antibodies protective? • • Antibodies at onset of outbreak and attack rate • Anti hev +ve0/46 ( 0%) • Anti hev –ve23/63( 37%) • Infusion of convalescent plasma into naïve animals induced protection against disease (but not infection) • In vitro neutralization of HEV by anti-HEV antibodies
Prevention • Improving sanitation is the most important measure • consists of proper treatment and disposal of human waste • higher standards for public water supplies • improved personal hygiene procedures • sanitary food preparation.
Best option to prevent hepatitis E infection • Clean drinking water
Immunoglobulin's in 3 rd. trimester reduces mortality • Immune serum globulin will considerably reduce mortality in the 3rd trimester of pregnancy
Vaccines At present, no commercially available vaccine
Vaccines on trial • Recombinant vaccine • Subunit vaccine
Recombinant vaccines • A 55 kDa recombinant HEV-derived ORF2 protein has been used to vaccinate rhesus monkeys • Although primates could still be infected, the vaccine protected them from the symptoms of disease
Subunit HEV vaccines • The direct intramuscular injection of purified plasmid DNA containing the full-length ORF2 of HEV has induced a prolonged humoral immune response (>12 months)
DNA immunization ORF2 was injected as an expression plasmid directly into muscle resulted in moderate anti- pORF2 titres in mice
Combined vaccine against hepatitis A and hepatitis E • Results showed that the combined vaccine could induce neutralizing antibodies against both hepatitis A virus (HAV) and hepatitis E virus (HEV) effectively in mice.