Patient presentation
Patient presentation. M. Vlooswijk, 16-2-2005. Content. Patient case and introduction Epidemiology Pathogenesis Clinical manifestations Diagnosis Treatment and prevention Prognosis Literature. Patient A. . Man, 46 years. Medical history: blank

Patient presentation
E N D
Presentation Transcript
Patient presentation M. Vlooswijk, 16-2-2005
Content • Patient case and introduction • Epidemiology • Pathogenesis • Clinical manifestations • Diagnosis • Treatment and prevention • Prognosis • Literature
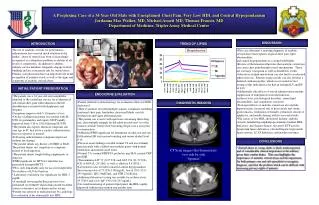
Patient A. • Man, 46 years. Medical history: blank • Symptoms: sudden onset of myalgia, diffuse upper and lower limb weakness, skin rash • During hospitalization: respiratory failure, prolonged ventilation and tracheostomy placement • Diagnostic tests: CSF and blood titers WNV +, EMG: widespread axonal loss of motor axons of upper and lower limb Source: Marciniak et.al. 2004
Patient A (II) • No improvement on intravenous immunoglobulin G • Complications: tracheobronchitis, pneumonia, Clostridium difficile infection and dysphagia requiring gastrostomy tube • Total hospital stay: 98 days • Rest impairment after rehabilitation: strength in upper limbs 2/3, lower limbs 2/2 Source: Marciniak et.al. 2004
Epidemiology • West Nile Virus, arbovirus, family Flaviviridae • First described in 1937 • Sporadic outbreaks in Israel and Africa • Mid-1990’s outbreaks with severe neurologic disease • First outbreak in North-America: NYC ‘99
Human cases of WNV infection in the USA, 1999–2003 Source: Lancet Infect Dis 2004
Bird-mosquito-bird cycle Source:Center for Disease Control and Prevention
Other ways of transmission: transfusion, organ transplants, transplacental, breast milk, percutaneous exposure in laboratory • 20% of infected persons develops mild illness • One:150 develops severe neurological illness • Peak incidence: August-September • In temperate climates possibly all year
Pathogenesis • Injection of virus-laden saliva • Infection of fibroblasts, vascular endothelial cells or cells of the RES viremia inflammation BBB CNS infection • Predilection within CNS: posterior thalamus, basal ganglia, brainstem, spinal anterior horn cells • Mechanisms of neuronal injury: acute neuronal necrosis, neuronophagia
Clinical manifestations Source: www.publichealthgreybruce.on.ca
Clinical manifestations (II) • Febrile illness: West Nile fever • Self-limited with fever, headache, malaise, back pain, myalgia and anorexia. Rash in 50% • Neuro-invasive disease • West Nile encephalitis • West Nile meningitis • Acute flaccid paralysis • Complications • Myocarditis, pancreatitis, hepatitis, ocular complications
Neuro-invasive disease • West Nile encephalitis • Encephalopathy, evidence of CNS inflammation, acute inflammation or demyelination on neuroimaging, focal neurological deficit, EEG consistent with encephalitis, seizures • West Nile meningitis • Clinical signs of meningeal inflammation, acute infection, acute meningeal inflammation on neuroimaging • Acute flaccid paralysis • Acute progressive limb weakness, asymmetry, hyporeflexia, no pain/paraesthesias or numbness, electrodiagnostic studies: anterior-horn-cell process, increased signal in anterior spinal grey matter on MRI
Diagnosis • To be considered in patients with unexplained febrile illness, encephalitis and/or meningitis, or flaccid paralysis, especially in summer or early fall. History of travelling to the US • Lab: • White bloodcell count in serum: normal or elevated • CSF: pleocytosis, predominance of lymphocytes, elevated protein concentration
Diagnosis (II) • Neuro-imaging: • CT: no evidence of acute disease • MRI: 30% enhancement of leptomeninges and/or periventricular areas, hyperintensity (T2) in basal ganglia, thalami, caudate nuclei, brainstem, spinal cord. • EEG: generalized continuous slowing • Electrodiagnostic studies: • Normal SNAP’s • Normal to markedly decreased CMAP’s
Diagnosis (III) • Serologic testing: • Detection of IgM antibody to WNV in serum or CSF, eg with MAC-ELISA • When IgM in CSF, CNS infection is highly probable • False-positive results: recent vaccination with yellow fever or Japanese encephalitis; recent infection with a related flavivirus (eg dengue)
Treatment and prevention • Supportive treatment • Trials: • iv immunoglobulin containing anti-WNV Ab • IFN alfa-n3 • Avoid exposure to mosquitoes (DEET) • Drainage of standing water • Blood donor screening for WNV • No human vaccines yet available
Prognosis • Mortality rates (associated with advanced age) • Encephalitis: 12% • Meningitis: 2% • Functional impairment • Acute flaccid paralysis: some improvement, no recovery • Encephalitis: difficulty walking, muscle weakness, cognitive impairment
Literature • Granwehr B.P. et.al. West Nile virus: where are we now? Lancet Infect Dis 2004; 4: 547-56 • Marciniak C. et.al. Acute flaccid paralysis associated with West Nile virus : motor and functional improvement in 4 patients. Arch Phys Med Rehabil 2004; 85: 1933-8 • Labowitz Klee A. et.al. Long-term prognosis for clinical West Nile virus infection. Emerging Infectious Diseases 2004; 10: 1405-11 • Petersen L.R. West Nile virus infection. UpToDate 2004