Download
1 / 49
490 likes | 609 Vues
Med K Patient Presentation December 5, 207. Craig Bayden Jeanne Rittschof. ID: 22 year old AA male with a headache. Past Medical History Significant for Migraines. Headache…. Started 2-3 days ago Increasing in severity- peaked this morning

E N D
Med K Patient PresentationDecember 5, 207 Craig Bayden Jeanne Rittschof
Headache… Started 2-3 days ago Increasing in severity- peaked this morning Entire head and neck hurts, especially with neck movement Mild Photophobia “I don’t think it’s a migraine”
And “Jock Itch” • Started before the headache • Red itchy bumps on scrotum and penis • Currently almost resolved
Additional Symptoms • Subjective Low Grade Fever • Mild Shortness of Breath • Generalized fatigue and weakness • Nausea and vomiting this morningED
Additional History • No pets • No sick contacts • Last Sexual Contact: 18 mos ago • No oral sex • No cold sores • No Known Allergies
Traveled to Korea in February • Camping retreat last week with exposure to wooded areas • no ticks • no mosquito bites
Medical and Surgical history • Heart murmur • Mild intermittent asthma • GERD • Migraines
Social History • College Student • Apartment with rooommate • City water • No Tobacco/No IVDU/No EtOH
Family History • Hypertension • Coronary Artery Disease • Diabetes Mellitus
Home Medications • Albuterol MDI PRN • Prilosec OTC • No other medicines including OTCs or Herbals
Vital Signs • BP 136/76 • HR 94 • RR 16 • T: 37.1C • 99% RA
General • Somnolent (ativan for LP)
Ocular Exam • Photophobia • PERRLA. • Extra Ocular Motions Intact • Sclera clear
ENT • Mucus Membranes Moist • Oropharynx without lesions or exudates
Neck • Limitted range of motion • No carotid Bruits • No thyromegally
Lymph Nodes • Bilateral Inguinal Adenopathy, tender, mobile • All other lymph nodes within normal limits
Cardiovascular • Regular Rate and Rhythm • II/VI systolic ejection murmur at LLSB, w/o radiation to carotids • Radial, Posterior Tibial, Carotids 2+ Bilaterally
Pulmonary • Clear to Auscultation Bilaterally • No consolidation on percussion • Respirations unlabored
Dermatology • No rashes • No petechiae • No bruises • See genitourininary
Genitourinary • Lesions covering scrotum and penis • Faint, small, circular, red papules • Non erupting, non crusting, non painful to palpation • No lesions around anus • Seemed to be resolving
Abdomen • Non distended • Positive bowel sounds • No hepatosplenomegally • Soft and non tender to palpation
Extremities • No cyanosis • No clubbing • No edema
Musculoskeletal • moves all extremities • Strength 4/5 (ativan) equal and bilateral • Cannot touch chin to chest
Neurological • Oriented x 3 • CN II-XII Intact • P2P, RAM, Rhomberg and Gait WNL • All DTRs 2+ bilaterally
CBC • WBC 7.5 • Hg 15.7/ Hct 47.6 • Platelets 214 • Absolute neutrophils 5.6 • Absolute lymphocyte count 1
Na 138 K 4.5 Cl 103 CO2 27 BUN 10 Creatinine 1.1 Glucose 94 Ca 9.5 Mg 2.1 Ph 3.3 BMP: Unremarkable
LFT’s • Tbili 0.6 • AST 82 • ALT 94 • Alk phos 67 • GGT 20
CSF • Clear, colorless • 231 nucleated cells • 84% Lymphocytes • Protein 76 • Glucose 49 • Atypical Lymphocytes
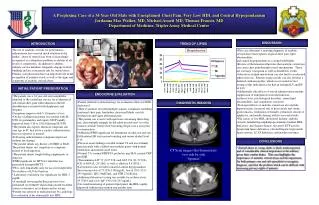
Imaging • Head CT: No acute intracranial process • RUQ US: No abdominal process • CXR: no air space disease
Initial Management • Vancomycin 1 gram IV Q12 hours • Ceftriaxone 2 grams IV Q12 hours • Acyclovir 800mg IV Q8 hours • Doxycycline 100mg IV Q12 hours
Studies Ordered • Blood cultures • Urine Cultures • CSF Cultures • HIV ELISA and Quantitative RNA • Rapid Influenza Assay • Serum RPR
Enterovirus PCR HSV PCR Adenovirus PCR VZV PCR CMV PCR EBV PCR VDRL Crypto Antigen Influenza Virus Additional CSF Studies
Diagnosis: aseptic meningitis with Varicella Zoster as causative pathogen.
Aseptic Meningitis Differential • Infectious: viruses, mycobacteria, fungi, spirochetes, tick borne • Drugs: NSAIDS, ATG, Sulfas, Quinolones and PCN • Malignancy • Autoimmune: Bechet’s, Mollaret’s • Partially Treated Meningitis
Viruses • Enterovirus • HSV 2 • HIV • LCMV • Mumps • CMV • EBV • VZV • Adenovirus • Arbovirus
Varicella Zoster • Human Herpes Virus • Causes Chicken Pox • Latent in cranial nerve and dorsal root ganglia • Reactivates causing a variety of manifestations
Reactivation manifestations • Shingles • Radiculoneuropathy • Ganglionitis • Post- herpetic neuralgia • Myelitis • Encephalitis/ Ventriculitis • Arteritis • Aseptic meningitis
Advent of PCR has increased awareness of VZV as a causative pathogen for viral meningitis.
One Finnish Study (2006) • 144 immunocompetent participants with aseptic meningitis • 66% had identifiable etiologies (PCR) for aseptic meningitis: • Enterovirus 26% • HSV2 17% • VZV 8% • 31% of patients with VZV mengingitis had no rash
References • Kupila, L et al. Etiology of aseptic meningitis and encephalitis in an adult population. Neurology 2006;66:75-80. • Gilden, D et al. Neurologic Complications of the Reactivation of Varicella-Zoster Virus. New England Journal of Medicine 2007;342: 635-646. • Up-To-Date (no access off campus)
Search PubMed • Aseptic Meningitis & Varicella Zoster Virus • Case Reports • Reviews • Drug Therapy