Download
1 / 35
350 likes | 823 Vues
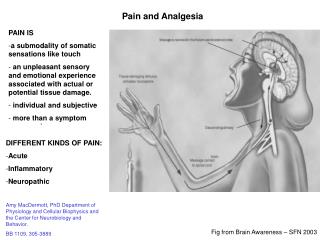
Identification of the Problem. Relates to the degree of effective pain control methodsPatient Controlled Analgesia (P.C.A.) Conventional Pain Control Intramuscular Injection (I.M.I.). PICO. P = Post-operative patientsI = Patient Controlled Analgesia (P.C.A.)C = Conventional pain control (I.M.I.)O = Pain management.

E N D
1. Fran Trujillo, R.N.
Mary Woods, R.N.
Edgar Paul, R.N.
Jeff Jeter, L.P.N.
OU College of Nursing
3. PICO P = Post-operative patients
I = Patient Controlled Analgesia (P.C.A.)
C = Conventional pain control (I.M.I.)
O = Pain management
4. Various Parameters &Populations Studied Ages > / = 7 to 72
Surgeries
Ethnicities & cultures
International
5. Interventions Patient Controlled Analgesia (P.C.A.)
Treatment for pain management
Intramuscular (I.M.) injection
Control group
Comparison treatment for pain management
6. Variables of Interest Dependent Variable ~ Pain
Independent Variable ~ Pain Control
P.C.A.
Conventional Pain Control (I.M.I.) There are other variables to consider as well: type of surgery, age, past pain experiences & preferences, culture & ethnicity, gender, disease process etc� There are other variables to consider as well: type of surgery, age, past pain experiences & preferences, culture & ethnicity, gender, disease process etc�
7. Burning Research Question
What is the best pain management practice for
post-operative patients; patient controlled
analgesia (P.C.A.) or conventional opioid
analgesia?
8. Literature Review Why is this a problem?
Lack of clinical evidence to support a change in practice
P.C.A. vs. I.M.I.
Threats to validity
Further research needed
(Hudcova, 2008)
9. Literature Review Why is this a problem?
Ineffective treatment of post-operative pain is documented
Various attitudes, beliefs, and cultures issues regarding pain
Pain symptoms are multi-faceted
Pain is invisible; often not assessed
Patient reluctance to report pain
Professionals have knowledge deficits and misconceptions about pain issues
(Yankova, 2008) (Bell, 2000)
10. Statistics P.C.A. weighted mean difference in pain intensity
8 points lower than control group 1st 24 hours
9 points lower than control group 25 to 48 hours
13 points lower than control group 49 to 72 hours
(Hudcova, 2008)
11. Mean Pain Scores (Carter-Snell, 1997)
12. P.C.A. Patient Satisfaction Reported pain control significantly higher
Ability to maintain near constant levels of analgesia
No peaks and troughs as with I.M.I.
Related to patient knowledge of P.C.A. & post-op experiences
Patient teaching crucial in optimal pain control
P.C.A. purpose & fear of addiction issues
(Yankova, 2008)
13. Mean Satisfaction Scores (Carter-Snell, 1997)
14. Review of Literature What has been done to study the problem?
Systematic Review
Research studies
15. Pros Found in Systematic Review
Patient preference for P.C.A.
Length of Stay (L.O.S.) ~ 0.4 days shorter
Clinically insignificant
Evidence to support P.C.A. efficacy
(Hudcova, 2008)
16. Pros Found in Studies Overwhelming evidence indicates P.C.A. provides superior analgesia resulting in less pain vs. I.M.I.
Patient autonomy and control
Self administering analgesia with P.C.A.
Exact & higher dosage vs. I.M.I.
No waiting for medication vs. I.M.I.
(Carr, 1997) (Conner, 1995)
(Carr, 1997) (Conner, 1995)
17. Pros Found in Studies
Evidence suggests P.C.A. provides more analgesia vs. I.M.I.
Some evidence suggests patients receiving I.M.I. report less pain
(Carr, 1997) (Conner, 1995)
18. Cons Found in Systematic Review
Clinical evidence does not support P.C.A. over conventional
pain control (I.M.I.)
P.C.A. patients may consume higher amounts of opioids
(Hudcova, 2008)
19. Cons Found in Studies The cost of P.C.A. higher
P.C.A. equipment
Opioids used
Differences in time cost insignificant between P.C.A. & I.M. groups
Some patients receiving I.M. injections reluctant to ask for pain medication
(Yankova, 2008) (Carr, 1997)
20. Cons Found in Studies
Null hypothesis supported: P.C.A. vs. I.M I.
Studies comparing P.C.A. vs. I.M.I. pain management provide inconclusive evidence supporting benefits of either
method for post-operative patients.
P.C.A provides inadequate pain relief after surgery
Pain level higher at rest & with exertion with I.M. injections
(Chang, 2004)
21. Cons Found in Studies Null hypothesis supported: P.C.A. vs. I.M.I.
I.M.I. dosages lower
Patient fear of I.M.I.
Nurse�s belief about pain management
Cost differences insignificant
(Chang, 2004)
22. Hudcova vs. Bronwyn Comparisons in findings
P.C.A. patients consume higher amounts of opioids
P.C.A. favored
Threats to validity
(Hudcova, 2008) (Bronwyn, 2005)
24. Hudcova vs. Chang Comparisons in findings
P.C.A. favored but inconclusive
P.C.A. patients had shorter L.O.S.
Threats to validity
(Hudcova, 2008) (Chang, 2004)
25. Hudcova vs. Carter-Snell Comparisons in findings
P.C.A. favored
Clinical evidence does not support P.C.A. over conventional pain control (I.M.I.)
Threats to validity
(Hudcova, 2008) (Carter-Snell, 1997)
26. Hudcova vs. Yankova Comparisons in findings
Inconclusive to rate P.C.A. over conventional pain control (I.M.I.)
Threats to validity
(Hudcova, 2008) (Yankova, 2008)
27. Results of Studies P.C.A. favored over Conventional (I.M.I.) Pain Management
Favored intervention for pain management
Patient satisfaction higher r/t lesser pain
Superior method of analgesia administration
Clinical statistics insignificant in terms of changing practice to PCA only. PCA favored but inconclusive. Either method inconclusive.
Clinical statistics insignificant in terms of length of stay.Clinical statistics insignificant in terms of changing practice to PCA only. PCA favored but inconclusive. Either method inconclusive.
Clinical statistics insignificant in terms of length of stay.
28. Results of Studies P.C.A. favored over Conventional (I.M.I.) Pain Management
Immediate access to higher & exact dosages
Pain ratings lower
Shorter length of stay in hospital
Patient education facilitated P.C.A. operation
Clinical statistics insignificant in terms of changing practice to PCA only. PCA favored but inconclusive. Either method inconclusive.
Clinical statistics insignificant in terms of length of stay.Clinical statistics insignificant in terms of changing practice to PCA only. PCA favored but inconclusive. Either method inconclusive.
Clinical statistics insignificant in terms of length of stay.
29. Pain Phenomena��..More Variables &
Is pain experienced differently in other cultures/environments?
Do men experience pain differently than women?
Do various types of surgery yield varying degrees of pain?
How do past experiences affect pain manifestations?
Do certain pain medications work better than others?
30. Patient Interventions
Effective pre-operative teaching on pain control method
Consider pain control experiences & preferences
Assess Pain
Rate pain
Administer analgesic as needed
31. Patient Interventions Monitor pain control effectiveness
Monitor Vital Signs
Re-assess pain
Rate pain
Music, touch, massage, relaxation, & imagery
Evaluate pain control method
32. Rationales Pain is subjective
Pain causes physiological & mental instability
Opioid analgesics may cause adverse side effects
Pain must be assessed and re-assessed for effective control
Pain must be evaluated for effective patient outcomes
33. Suggestions for Further Study Nurses play key role in pain management
Continuing education is pivotal
Clinical practice is a constantly changing environment
Patient and care provider education positively influences pain management
(Johnston, 1993)
34. Suggestions for Further Study Compare & contrast various opioids per
Patient history
Dosage
Surgical procedure
Disease process
35. References Bronwyn, E. (2005). Differences in postoperative opioid consumption in patients prescribed patient-controlled analgesia (PCA) versus intramuscular injection. American Society for Pain Management Nursing. 6 (4),137-144.
Carter-Snell, C., Fothergill-Bourbonnais, F., Durocher-Hendriks, S. (1997). Patient controlled analgesia and intramuscular injections: a comparison of patient pain experiences and postoperative outcomes. Journal of Advanced Nursing 25(4),681-690).
Chang, A.M., Ip, W.Y., Cheung, T.H. (2004). Patient-controlled analgesia (PCA) versus conventional intramuscular injection (I.M): a cost effective analysis. Journal of Advanced Nursing, 46(5), 531-541.
Hudcova, J., McNicol, E.D., Quah, C.S., Lau, J., Carr, D.B. (2008). Patient controlled analgesia versus conventional opioid analgesia for postoperative pain (review). The Cochrane Collaboration Issue (4), 1-73.
Yankova, Z. (2008). Patients� knowledge of patient controlled analgesia (PCA) and their experiences of postoperative pain relief: a review of the impact of structured preoperative education. Journal of Advanced Perioperative Care, 3(3), 91-99.