The Electronic Health Record
The Electronic Health Record. Willa Fields, RN, DNSc , FHIMSS. Outline. Patient Medical Records Paper and Electronic Nursing Terminologies Bar Code Medication Administration Computerized Physician Order Entry Clinical Decision Support Picture Archiving Communication System Usability

The Electronic Health Record
E N D
Presentation Transcript
The Electronic Health Record Willa Fields, RN, DNSc, FHIMSS
Outline • Patient Medical Records • Paper and Electronic • Nursing Terminologies • Bar Code Medication Administration • Computerized Physician Order Entry • Clinical Decision Support • Picture Archiving Communication System • Usability • Downtime • 2009 American Recovery and Reinvestment Act
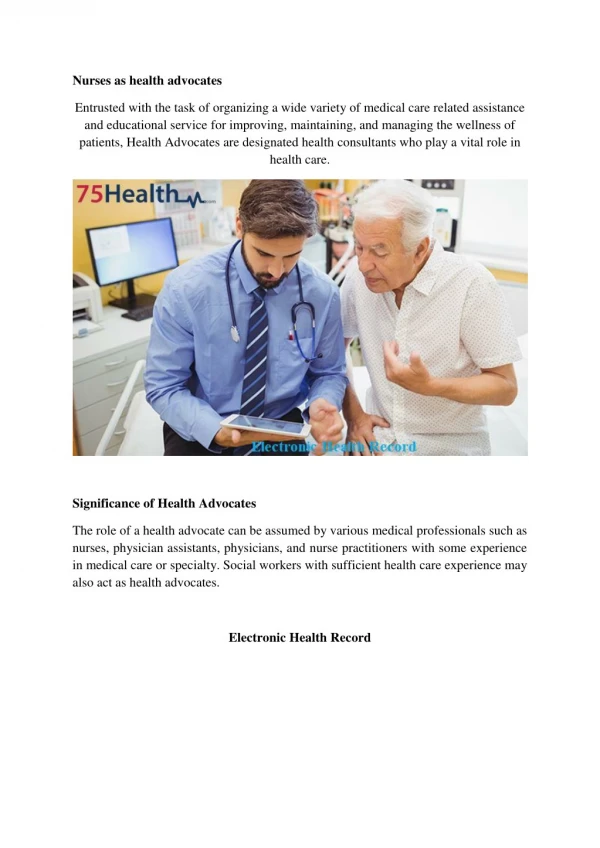
Purpose of Patient Record (electronic or paper based) • Memory cue for provider • Communication vehicle among care providers • Longitudinal “story” of patient’s care • Risk Management • Reimbursement • Quality Improvement
Paper Health Care Records • Ease of use • Only one version • Can be locked up; easily secured • Comfortable – “how we have always done it”
MGH Problems with Paper Health Care Records • Difficulty accessing chart • Incomplete records • Illegible entries • Loss of time for transcription • Time consuming data collection • Duplicate data entry • Not “Searchable” • “Weeding” thick charts • Can’t tell who has viewed record • Storage needs
Health Care Information Systems • Business Systems • Admission, Discharge, Transfer (ADT) • Financial Systems • Acuity Systems • Scheduling Systems • Communication Systems • Call light systems • Wireless phones, pagers • Email, instant messaging
Clinical Information Systems • Order Entry Systems • Clerk entered • Provider entered • Documentation Systems • Pharmacy Systems • Laboratory Systems • Radiology Systems • Data Systems • Data warehouse • Data mining • Case Management Information Systems • Decision Support • Care plan
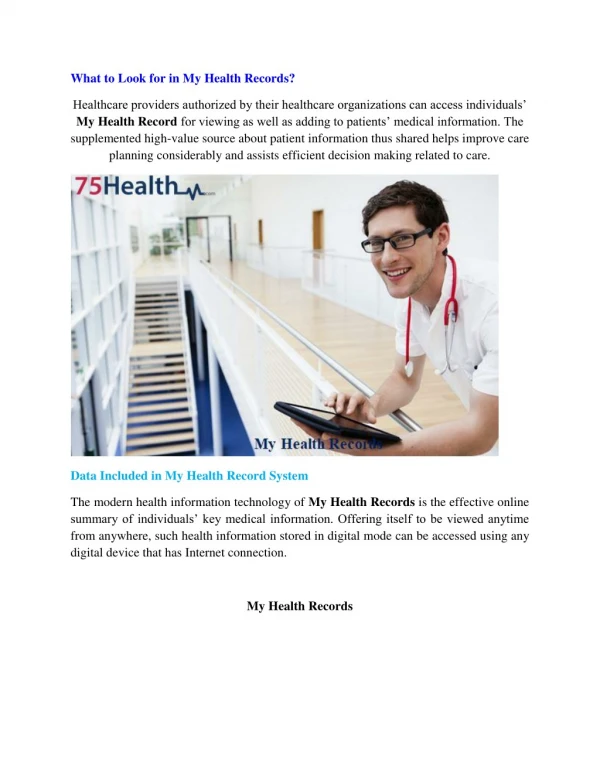
Electronic Health Record (EHR) • Longitudinal electronic record of patient health information generated by one or more encounters in any care delivery setting. • Included in this information are patient demographics, progress notes, problems, medications, vital signs, past medical history, immunizations, laboratory data and radiology reports. http://www.himss.org/asp/topics_ehr.asp
ABCs of Electronic Records • Electronic Medical Record (EMR) • Computerized Patient Record (CPR) • Clinical Information System (CIS) • Electronic Health Record (EHR) • Personal Health Record (PHR) • ???
Why EHRs are Important • Health Maintenance • Trend Analysis • Alerts • Decision Support The promise of improved patient safety
Institute of Medicine (IOM): Eight EHR Core Functions • Health Information and Data • Results Management • Order Management • Decision Support • Electronic Communication and Connectivity • Patient Support • Administrative Processes and Reporting • Reporting and Population Health
Nursing Terminologies Purpose Examples Clinical Care Classification (CCC) International Classification of Nursing Practice (ICNP) North American Nursing Diagnosis Association International (NANDA) Nursing Intervention Classification (NIC) Nursing Outcome Classification (NOC) Omaha Home Health Care System Perioperative Nursing Data Set (PNDS) • Common language that will help quantify the unique contribution and impact of nursing • Help convey an understanding of nursing to others • Are imbedded in EHRs and often transparent
EMR Adoption Model http://www.himssanalytics.org/hc_providers/stage6Hospitals.asp
United States EHR Use • Surveyed 3000 USA hospitals in 2008 • 1.5% use comprehensive EHRs • 7.6% use basic EHRs in at least one unit that includes physician and nurse progress notes • 17% have widely available CPOE • Large, urban, teaching hospitals most likely to afford EHRs • Conclusion: “IT adoption levels are abysmally low in American hospitals.” Jha, A. et al. (2009) Use of electronic Health Records in US Hospitals. New England Journal of Medicine (DOI: 10:1056/NEJMsa0900592)
International Use of EHRs http://www.itif.org/files/2009-leadership-healthit.pdf
N=5166 N=5235 Current EMR Usage N=5166 N=5233 N=5281 http://www.himssanalytics.org/
Clinical Documentation • Medication Administration Record (MAR) • Vital Signs • Interdisciplinary Notes
Safeguarding Medication Process • 49% errors during ordering phase • CPOE helps reduce incidence • 25% errors during processing • Robotics helps reduce incidence • 26% errors during administration • Bedside bar coding helps reduce incidence Bates et al: JAMA 1995; 274:29-34
Common Medication Ordering Errors • Wrong medication for condition • Wrong dose, route, interval, duration • Allergies • Drug/Drug interactions • Drug/laboratory interactions • Transcription errors
Safeguarding Prescribing Process • 30% errors due to lack of knowledge of medication ordered • 29.2% errors from lack of knowledge of effects of patient factors on medication ordered • 17.5% errors from wrong calculations, decimals, rates, units, etc • 13.4 % from nomenclature factors Lesat TS et al: JAMA 1997; 277: 312-317
The Bar-coding Medication Administration System (BCMA) Scanner linked wirelessly to Electronic Medication Administration Record (eMAR) Patient receives bar-coded armband All caregivers have bar-coded ID badges Scan badge, patient armband and medication Administer medication safely!!!
Scanning the patient’s armband Image retrieved from http://www.psqh.com/mayjun07/improvingsafety.html
Limitations of the BCMA Very expensive to bar code all pharmaceuticals! STAT drugs, over ride drugs (i.e. hypoglycemic protocol) Downtime procedures Pt’s armband falls off/lost Ordered Dose does not match dispensed dose Hardware issues (dead batteries) User Issues (staff compliance) Multi-dose vials Cost
Benefits of the BCMA • Reduction in overall medication errors, adverse drug events, enforces the 5 medication administration rights • Better inventory control • Can see when patient received medications • Patient feels safer • Less litigation cases = Happy RN • JCAHO National Patient Safety Goals
Veterans Administration Experience • Medication errors reduced • Dispensing error- 31% • Risk for potential adverse drug events 63% • Incorrect medication- 58% • 53% decrease in incorrect dose and strength of a medication • 100% elimination of incorrect dosage forms
Computerized Physician Order Entry (CPOE) • Clinical software application designed specifically for physicians to write patient orders electronically rather than on paper • Potential to dramatically reduce errors, especially medication errors • Configured for individual orders or order sets
Pick Item To Order. Click Process Order
Getting Physicians to Use Computers • Many physicians are not computer literate • System must be quick and easy to use • System must increase overall physician efficiency • Tailor training to meet varied physician needs • Respond to issues quickly • Need physician champions
American College of Physician Executives CPOE Survey Comments: “worst aspect of my 25 years in medicine… has ruined doctor productivity, produced lower quality of care… http://www.healthcareitnews.com/news/docs-may-be-using-it-they-dont-love-it
Clinical Decision Support • Rules that assist the clinician in entering complete, accurate, and appropriate patient care orders • Drug/drug interactions • Drug allergy conflicts • Minimum/maximum drug dosing parameters • Duplicate orders • Digoxin and potassium levels • Antibiotics and renal function
Results Viewing • Laboratory • Radiology • Transcriptions • Vital Signs • Fetal monitoring • Cardiac monitoring