RAC Appeal Process Strategies
RAC Appeal Process Strategies. Patrick C. Devine, Jr. Courtney A. Miller. Demonstration Results. RACs identified $1.03 billion in improper payments 96% of identified improper payments = overpayments After appeals, etc., $693 million returned to Medicare Trust Fund

RAC Appeal Process Strategies
E N D
Presentation Transcript
RAC Appeal Process Strategies Patrick C. Devine, Jr. Courtney A. Miller
Demonstration Results • RACs identified $1.03 billion in improper payments • 96% of identified improper payments = overpayments • After appeals, etc., $693 million returned to Medicare Trust Fund • 34% of provider appeals successful
Demonstration Project • Take Aways: • Take steps to limit exposure for improper payment claims • Before a RAC review • Understand the review and appeals process if subject to RAC review
Limit Exposure • Develop a RAC Response Team Now • Include members from all areas of risk • On-going duties • Team responsible for entire RAC process • Assessing areas of risk • Keeping track of all record requests • Implementing compliance strategies • Handling all RAC reviews and appeals from start to finish • Key person for all RAC communications
Limit Exposure • Educate staff on Medicare billing issues • Focus on areas of known weaknesses • Learn from colleagues, the Demonstration Project and other sources • Medical necessity • Coding errors • RAC Status Documents (www.cms.gov/rac) • OIG Work Plan
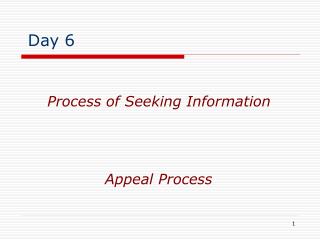
Audit Areas and Top Error by Provider Type Source: Medicare RAC Program: An Evaluation of the 3-Year Demonstration
Limit Exposure • Self Audits • Self Disclosure • Important to work with legal counsel • Legal obligations • Process for Voluntary Refunds • Benefits and Consequences • Voluntary refunds will exclude the claims from RAC review
Overview of the RAC Review/Appeal Process • RAC Review • Initial Determination • Recoupment • Informal Appeal: Rebuttal • Formal Appeal • 5 levels
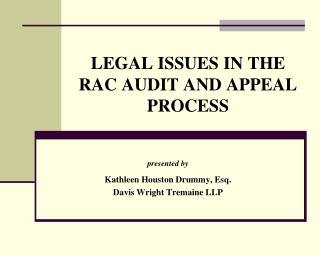
Overview of Review and Appeals Process Source: American Hospital Association
RAC Review • 2 Types of reviews • Automated (software searching for clear errors) • Complex (review of patient records) • RAC’s authority to request records is subject to limits • All requests should be channeled through RAC Team
RAC Review • Provider must provide requested records within 45 days • Failure = RAC authorized to find improper payment • Failure = potential loss of right to appeal • RAC Team should control this process • Extensions possible
Initial Determination • RAC’s Initial Determination • Timeframe for RAC determination • 60 days after receiving records • Failure to respond = ??? • Possible defense • Written notice to provider • Reason for denial
Recoupment • If RAC identifies overpayment, Medicare typically uses recoupment to recover • Begins 41 days after date of demand • Provider can delay recoupment until the 3rd stage of appeal process • Deadlines: appeal v. delay of recoupment • After Reconsideration stage, provider can delay recoupment through an extended repayment plan
Recoupment & Interest • Interest accrues from date of final determination, unless paid within 30 days • Continues to accrue during appeal process • Fixed interest rate (currently 11.38%) • Factor to consider before appealing • Pay and then appeal?
Rebuttal • Provider can rebut RAC’s initial determination • File with RAC within 15 days after receipt • When to consider: New documentation to support the claim • Not required • Does NOT toll deadline for filing formal appeal
Formal Appeals Process • 5 Levels (Medicare Appeals Process) • Redetermination • Reconsideration • Administrative Law Judge Hearing • Medicare Appeals Council Review • Federal Court
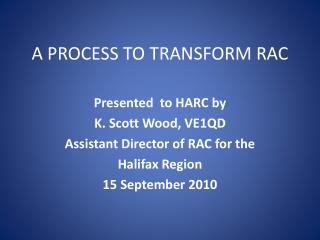
FI, carrier 60 days+14 day extension 180-194 Days Notice Letter 120 Days to File 180 Days to File 240 Days QIC 60-day time limit 60 Days to File 780- 794 Days 150 Days ALI 90-day time limit 60 Days to File 150 Days MAC 90-day time limit 60 Days to File US District Court Last Level- No time limit 60+ Days Appeals Timeline
Results of the Demonstration • Connelly v. Viant??
Factors to Consider • Time • Cost of appeal • Resources • Quality of documentation • Implications • Clinical support • Legal involvement
Outcomes • Full Reversal • No further action, RAC cannot appeal • RAC must refund contingency fee • Provider may be paid interest • Partial Reversal • Denial
Level 1: Redetermination • File request for redetermination with FI • If not inpatient hospital, then with Carrier • Rebuttal not required • Must file within 120 days of receipt of RAC determination • Exception for “Good Cause”
Level 1: Redetermination • Request must be in writing • Use CMS form 20027 or develop your own • Provide evidence explaining why provider disagrees • Raise all issues and submit all relevant documents • No hearing, decision based on written appeal
Level 1: Redetermination • No minimum requirements for amount in controversy • FI has 60 days to approve/reverse initial determination
Level 2: Reconsideration • File with Qualified Independent Contractor (“QIC”) • Virginia = Maximus • Must file within 180 days after receipt of notice of Redetermination • Use CMS Form 20033 or develop your own
Level 2: Reconsideration • Written appeal; no appearance necessary • Raise all issues and submit all evidence • If not, excluded from consideration in subsequent appeals • No minimum amount of controversy
Level 2: Reconsideration • QIC conducts an independent, on the record review • Medical necessity reviewed by panel of MDs • QIC authority • Must follow LCDs, CMS rulings, laws
Level 2: Reconsideration • Within 60 days of receipt of request, QIC must mail written notice of action: • Reconsideration • Inability to complete the reconsideration • Dismissal of claim • If QIC fails to act within 60 days, provider may appeal to ALJ
Level 3: ALJ Hearing • Must be filed within 60 days of receipt of notice of QIC’s reconsideration • Use CMS Form 20034A • $120.00 min. amount in controversy • Hearing typically by tele-conference • Usually within 90 days • Develop good oral testimony • No new evidence
ALJ Hearing • Evidence is limited to what was presented for reconsideration (QIC) • Exception for good cause • ALJ can subpoena witnesses/documents • ALJ will consider all issues previously considered
ALJ Hearing • Within 90 days of the hearing, ALJ must issue written decision • Remand to QIC • Dismissal • Approve
Level 4: MAC Review • Must file request within 60 days after receipt of ALJ’s decision • MAC may review ALJ decision on its own motion or based on referral by CMS • MAC will issue its final decision within 90 days of receipt of request for review
Level 4: MAC Review • MAC reviews the ALJ’s decision de novo • Limited to the evidence in the ALJ’s administrative record • In some cases, briefs requested • No right to a hearing • MAC may adopt, reverse, modify or remand the case to ALJ
Level 5: Federal Court • File appeal within 60 days of receipt of MAC’s decision • Min. amount in controversy - $1,220 • File in USDC in the provider’s district
Level 5: Federal Court • Limited purpose: questioning the decision of the MAC and the findings of the ALJ • Evidence limited to ALJ record • No deadline for decision • No appeal from this level • Entire process can take up to two years
Appeal Strategies • Advocate the Merits • Treating Physician Rule • Waiver of Liability • Provider Without Fault • Reopening Not Based on Good Cause • Challenging the Statistics • Constitutional Challenge
Advocating the Merits • Not technically a “defense” • Factual and legal arguments supporting payment • Prepare position paper • Use qualified expert to confirm medical necessity
Treating Physician Rule • Medical necessity • Treating physician in the best position to judge • Physician’s determination should be given more weight than RAC • RAC uses medical professionals who have never met or assessed the patient
Waiver of Liability • Medical Necessity • Section 1879(a) of the Social Security Act • Payment permitted if provider “did not know, and could not reasonably have been expected to know, that payment would not be made for such services”
Waiver of Liability • Maintain records of all communications with Medicare representatives • i.e. Overpayment claim overturned in past
Provider Without Fault • Medical Necessity • Section 1870 of the Social Security Act • Provider entitled to payment when the provider is without fault and denial of the claim is deemed be against equity and good conscience
Provider Without Fault • Generally, provider considered to be without fault if: • Exercised reasonable care • Made full disclosure of all material facts • Had a reasonable basis for assuming payment was correct
Provider Without Fault • Considers various factors • Age, linguistic limitations, etc. • Document phone calls, guidance from CMS or carrier. • Individual communications • General communications to provider and supplier community
Reopening Not Based on Good Cause • RACs must adhere to regulatory timeframes for reopening initial determinations • For Medicare generally: • Within 1 year – for any reason • Within 4 years – for good cause • No deadline if reliable evidence of fraud • RAC limited 3-year look-back period • Only back to October 2007
Reopening Not Based on Good Cause • Good Cause: • New and material evidence (not readily available or known) OR • Obvious error made at the time of determination • Recent Transmittal: A contractor’s decision to reopen based on the existence of good cause, or refusal to reopen after determining good cause does not exist, is not subject to appeal.
Challenging the Statistics • RACs may extrapolate in certain circumstances • Must follow Medicare’s statistical guidelines • Use a third party expert to challenge the validity of the extrapolation
Constitutional Challenge • Possible Argument?
Conclusion • Take steps to prepare NOW • Establish a RAC Team • Limit exposure • Maintain adequate records • Appeals process • Deadlines • Defenses
Questions • Patrick C. Devine, Jr. pdevine@williamsmullen.com757.629-0614 • Courtney A. Miller cmiller@williamsmullen.com 757.629.0665