Download
1 / 43
480 likes | 861 Vues
Focus on Peripheral Arterial Disease of the Lower Extremities. (Relates to Chapter 38, “Nursing Management: Vascular Disorders,” in the textbook). Peripheral Arterial Disease Description. Involves progressive narrowing and degeneration of arteries of neck, abdomen, and extremities

E N D
Focus on Peripheral Arterial Disease of the Lower Extremities (Relates to Chapter 38, “Nursing Management: Vascular Disorders,” in the textbook)
Peripheral Arterial DiseaseDescription • Involves progressive narrowing and degeneration of arteries of neck, abdomen, and extremities • Atherosclerosis is the leading cause of majority of cases
Peripheral Arterial DiseaseDescription • Typically appears at ages 60s to 80s • Largely undiagnosed • Risk factors • Cigarette smoking • Hyperlipidemia • Hypertension • Diabetes mellitus
Peripheral Arterial DiseaseClinical Manifestations • Classic symptom of PAD—intermittent claudication • Ischemic muscle ache or pain that is precipitated by a constant level of exercise • Resolves within 10 minutes or less with rest • Reproducible
Peripheral Arterial DiseaseClinical Manifestations • Paresthesia • Pain at rest • Occurs in the forefoot or toes and is aggravated by limb elevation • Occurs from insufficient blood flow • May indicate critical ischemia
Peripheral Arterial DiseaseClinical Manifestations • Thin, shiny, and taut skin • Loss of hair on the lower legs • Diminished or absent pedal, popliteal, or femoral pulses • Pallor
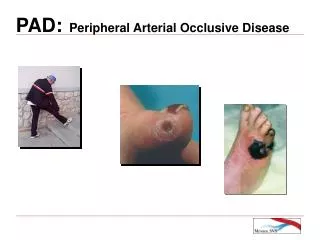
Peripheral Arterial DiseaseComplications • Atrophy of the skin and underlying muscles • Delayed healing • Wound infection • Tissue necrosis • Arterial ulcers
Peripheral Arterial DiseaseComplications • Nonhealing arterial ulcers and gangrene are most serious complications • May result in amputation if blood flow is not adequately restored or if severe infection occurs
Peripheral Arterial DiseaseComplications • Arterial Ulcers (see table 38-2) • Small, deep, round “punched out” appearance • Minimal drainage • Typically occur on tips of toes or feet • Ulcer tissue may have black eschar or pale pink granulation
Peripheral Arterial DiseaseDiagnostic Studies • Doppler ultrasound • Segmental blood pressures • Ankle–brachial index (ABI) • Done using a handheld Doppler • Angiography • Magnetic resonance angiography (MRA)
Collaborative CareRisk Factor Modification • Smoking cessation • Aggressive treatment of hyperlipidemia • Hypertension and diabetes mellitus • BP maintained <130/80 • Glycosylated hemoglobin <7.0% for diabetics
Collaborative CareDrug Therapy • Antiplatelet agents • Aspirin • Ticlopidine (Ticlid) • Clopidogrel (Plavix) • ACE inhibitors
Collaborative CareDrug Therapy • Drugs prescribed for treatment of intermittent claudication • Pentoxifylline (Trental) • ↓ Blood viscosity • Cilostazol (Pletal) • ↑ Vasodilation
Collaborative CareExercise Therapy • Exercise improves oxygen extraction in the legs and skeletal metabolism • Walking is the most effective exercise for individuals with claudication • 30 to 60 minutes daily
Collaborative CareNutritional Therapy • Dietary cholesterol <200 mg/day • Decreased intake of saturated fat • Soy products can be used in place of animal protein
Collaborative CareCare of Leg with Critical Limb Ischemia • Protect from trauma • Reduce vasospasm • Prevent/control infection • Maximize arterial perfusion • Other strategies • Immune modulation therapy • Angiogenic gene therapy
Collaborative CareInterventional Radiologic Procedures • Indications • Intermittent claudication symptoms become incapacitating • Pain at rest • Ulceration or gangrene severe enough to threaten viability of the limb
Collaborative CareInterventional Radiologic Procedures • Percutaneous transluminal balloon angioplasty • Involves the insertion of a catheter through the femoral artery • Balloon is inflated dilating the vessel by cracking the confining atherosclerotic intimal shell
Collaborative CareSurgical Therapy • Most common surgical approach • A peripheral arterial bypass operation with autogenous vein or synthetic graft material to bypass blood around the lesion
Collaborative CareSurgical Therapy • Endarterectomy • Patch graft angioplasty • Amputation
Nursing ManagementNursing Assessment • Past health history • Diabetes mellitus • Smoking • Hypertension • Hyperlipidemia • Obesity
Nursing ManagementNursing Assessment • Exercise intolerance • Loss of hair on legs and feet • Decreased or absent peripheral pulses
Nursing ManagementNursing Diagnoses • Ineffective tissue perfusion (peripheral) • Impaired skin integrity • Activity intolerance • Ineffective therapeutic regimen management
Nursing ManagementPlanning • Overall goals for patient with PAD • Adequate tissue perfusion • Relief of pain • Increased exercise tolerance • Intact, healthy skin on extremities
Nursing ManagementNursing Implementation • Health Promotion • Identification of at-risk patients • Community involvement • Diet modification
Nursing ManagementNursing Implementation • Acute Intervention • Frequently monitor after surgery • Skin color and temperature • Capillary refill • Presence of peripheral pulses distal to the operative site • Sensation and movement of extremity
Nursing ManagementNursing Implementation • Acute Intervention • Continued circulatory assessment • Monitor for potential complications • Knee-flexed positions should be avoided except for exercise • Turn and position frequently
Nursing ManagementNursing Implementation • Ambulatory and Home Care • Management of risk factors • Importance of meticulous foot care • Importance of gradual physical activity after surgery
Nursing ManagementNursing Implementation • Ambulatory and Home Care • Daily inspection of the feet • Comfortable shoes with rounded toes and soft insoles • Shoes lightly laced
Nursing ManagementEvaluation • Identify activities that promote circulation • Maintain adequate peripheral tissue perfusion • Experience intact skin, free of infection, on lower extremities
Nursing ManagementEvaluation • Plans for walking program • Increased activity tolerance • Verbalize key elements of therapeutic regimen, knowledge of disease, treatment plan, reduction of risk factors, and proper ulcer/foot care
Venous Thrombosis Factors in venous thrombosis (38-7) 1. Venous stasis 2. Endothelial damage 3. Hypercoagulability
Superficial Thrombosis • Manifestations • Palpable cord • Red, warm , tender skin • Mild temperature elevation • Possible edema • Care • Elevation • Heat, • Analgesics
Deep Vein Thrombosis (DVT) • Manifestations • Unilateral edema • Pain • Warm skin • Fever • Positive Homan’s sign (caveat) • May be minimally symptomatic
DVT • Potential Complications • Pulmonary embolism • Chronic venous insufficiency • Diagnosis • Doppler
DVT • Prevention oand prophylaxis • Anticoagulation • Prevention AND treatment • Lovenox, heparin, fondaparinux • Coumadin
DVT • Nursing Interventions • Management and teaching related anticoagulation • Safety • Monitoring • Diet • Minimization of bleeding risk • Education about signs/symtpoms of PE
Chronic Venous Insufficiency • A condition in which the valves of the veins are damaged---> retrograde blood flow, pooling of blood in the legs. • May lead to venous stasis ulcers
Chronic Venous Insufficiency • Manifestations • Brawny skin, possible eczema • Edema , possible severe • Venous ulcers • Tend to occur above medial malleolus • Weepy, - extensive drainage • shallow, irregular shaped • Larger than arterial ulcers
Chronic Venous Insufficiency • Care of ulcers • Compression of venous insufficiency *avoid if concurrent PAD Moist dressings Balanced diet with adequate protein, vitamins A/C Antibiotics if infection is present

![Diffuse Vascular Disease (Focus on Peripheral Arterial Disease [PAD])](https://cdn1.slideserve.com/3363465/slide1-dt.jpg)