Download
1 / 38
410 likes | 1.2k Vues
Pregnancy & Prenatal Care. Jennifer McDonald DO. What is the purpose of prenatal care?. WHEN SHOULD PRENATAL CARE START?. History. Routine prenatal care relatively new 1900 the nurses of the instructive nursing association in Boston began making house calls to pregnant mothers

E N D
Pregnancy & Prenatal Care Jennifer McDonald DO
History • Routine prenatal care relatively new • 1900 the nurses of the instructive nursing association in Boston began making house calls to pregnant mothers • Noticed that complications were decreased. Ultimately practice adopted by physicians
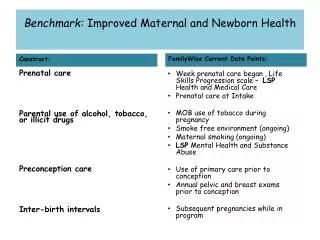
IDEALLY, a woman planning to have a child should have a medical evaluation before she becomes pregnant The majority of pregnancies are unintended making pre-conceptual care challenging 25% of pregnancies worldwide will end in a termination
Always Terminology Embryo (Greek “swelling within”) Fertilization thru 8 weeks Fetus (Latin “Offspring”) Beyond 8 weeks through delivery Neonatal period = birth until 28 days of life
Terminology • Premature infant < 37 weeks gestation • Post-mature infant > 42 weeks gestation • Low birth weight < 2500 grams at birth • Macrosomic infant > 4500 grams at birth • Spontaneous Abortion = expulsion of an infant prior to 20 weeks of gestation • Viability = 23-24 weeks gestation
Gravity & Parity Gravity = Total number of pregnancies Parity = Outcome of pregnancies • Sometimes expressed as 4 digits Full term deliveries Preterm deliveries Abortions (spontaneous or elective) Living children • A multiple birth is a single parous experience
Numbers Game • Nulligravid = never been pregnant • Primigravid = first pregnancy • Multigravid = achieved previous pregnancies
Duration of Pregnancy • Calculated from the first day of the last menstrual period (LMP) • Average 280 days (40 weeks)
Numbers Game Naegele’s Rule EDC = LMP - 3 months + 7 days Example LMP 5/21 is due ??
Diagnosis of Pregnancy • Presumptive Signs • Probable Signs • Positive Signs
Presumptive • Secondary amenorrhea • Nausea & vomiting • Breast changes • Skin changes (cholasma/linea nigra) • Urinary frequency • Fatigue • Quickening (first perception of fetal movement)
Probable Signs • Abdominal enlargement – uterus rises out of the pelvis at 12 weeks • Braxton Hicks contractions • Uterine souffle – rushing of maternal blood in placenta • Goodell’s sign – softening of cervix 6-8 weeks • Chadwick’s sign – bluish hue to cervix after 6 weeks • Fetal movement – felt 18 to 20 weeks, earlier in multigravidas (14-16 weeks)
Positive Signs • Fetal heart tones heard • Identifiable with doppler after 10 weeks • Fetus identified on ultrasound • Palpation of the fetus (22 weeks) • Positive hCG • Now able to be identified up to 4 days before missed period
Estimating Gestational Age • Uterus palpable at pubic symphysis at 8 weeks • Rises out of pelvis at 12 weeks • Mid to umbilicus at 15 weeks • At umbilicus at 20 weeks • Fundal height correlates with gestational age from 26-34 weeks
Fundal Height Measured from pubic symphysis to uterine fundus Should measure +/- 2 cm compared to weeks gestation
Ultrasound Early Landmarks • 5 weeks Chorionic sac; yolk sac • 6 weeks Yolk sac/embryo; cardiac activity • 7 weeks Embryonal movement • 8 weeks Extremities visible Measurement < 12 weeks = crown rump length hCG Levels GS = 1000-1200 Yolk sac = 7200 Embryo/cardiac activity = 10,800 Fetal loss rate after finding cardiac activity is 5%
Ultrasound • After 12 weeks Head circumference Biparietal diameter Femur length Abdominal circumference
The First Visit • Present pregnancy • Establish dating • Previous pregnancy history • Complications, routes of delivery, etc. • Medical/Social history • Surgical history • Previous gyn surgery very important • Family history
Teratogens Cigarette Smoking • Only 20% of patients quit during pregnancy • Low birth weight, increased risk of fetal death, placental abruption, placenta previa
Alcohol Exposure • Alcohol crosses easily across the placenta • One of leading causes of mental retardation • Facial abnormalities • Cardiovascular defects • CNS dysfunction
Fetal Alcohol Syndrome (1)CNS dysfunction low intelligence microcephaly behavioral abnormalities (2)Growth restriction (3) Facial anomalies (4) Congenital heart defects Daily ETOH not as important as max concentration at critical periods
FAS 3rd leading cause of birth defects
Significant Maternal Disorders • Seizure disorders • Pre-gestational diabetes • Cardiac disease • Psychiatric disorders • Thyroid disease
Initial Routine Lab Evaluation • CBC • Blood type & antibody screen • Rubella • Hepatitis B • RPR (serologic test for syphilis) • HIV (not mandatory) • Urinanalysis
Genetic Screening • Advanced maternal age > 35 years old • Cystic fibrosis screening • Sickle cell screening • Hemoglobinopathies • TaySachs Ashkenazi Jewish (1 in 27 carriers) Baseline risk of major congential malformations is 3.4% Baseline risk for genetic disorders is 0.5%
Prenatal Diagnosis Chorionic villous sampling (CVS) Amniocentesis
Frequency of Visits • Monthly until 30 weeks • 30-36 weeks every 2 weeks • 36 weeks to delivery every week Every visit: Weight/blood pressure Urine dip: protein/glucose Fetal heart tones/fundal height Labor symptoms/Hypertension symptoms
Other Testing • Routine screening GC/chlamydia • Pap smear • Glucose challenge test • 28 weeks • 50 gram load/Not fasting/1 hour > 135 indicates need for 3 hour test • Group B Strep (36 weeks)
Glucose Challenge Test • Used for diagnosis when screening test (1 hour) abnormal • Overnight fast/100 gram load • Two or more abnormal values • Fasting > 95 mg/dL • 1 hour > 180 mg/dL • 2 hour > 155 mg/dL • 3 hour > 140 mg/dL
Rubella • Infection can be communicated 7 days before and 4 days after rash appears • If develops will be 2-3 weeks after exposure • Rate of infection depends on trimester < 11 weeks = 90% chance congenital infection 11-12 weeks = 33% 13-14 weeks = 24% 15-16 weeks = 11% >16 weeks = Less than 1%
Contraindicated measles mumps rubella yellow fever Case Dependent polio influenza rabies hepatitis A/B pnuemococcal tetanus toxoid Vaccinations in Pregnancy
HIV Testing • ACOG recommends testing for all pregnant women • AZT in pregnancy and labor decreases transmission from 25% to 8% • Scheduled C-section (before onset of labor) decreases transmission to 2% • IV AZT 3 hours prior to c-section • Avoid amniocentesis or other invasive procedures • Viral load at baseline and every 3 months • Breast feeding contraindicated
Group B Streptococcus • Leading cause of life threatening perinatal infection • 15-30% women asymptomatic carriers • Early onset (80% within 6 hours of delivery) carries 6% chance neonatal mortality • GBS bacturia on initial urinanalysis implies heavy bacterial load • Routine screening perfomed 34-36 weeks • Prophylaxis at delivery if positive
Quad Screen • Screening for Down’s, neural tube defects, Trisomy 18 • 16-20 weeks Detection with ultrasound 60-70% 60% 75-80%