Download
1 / 26
280 likes | 315 Vues
Explore the essentials of parenteral nutrition (PN) and its application in cancer patients as discussed by Dr. Osman Abbasoğlu, a Professor of Surgery at Hacettepe University. Learn about the role of PN, ways of delivering PN, requirements for PN in cancer, complications, and supporting PN safety. Gain insights from the valuable personal experience shared. This informative session also addresses the use of PN in gastrointestinal dysmotility, surgical patients, and critical illness situations. Consider the benefits and challenges of PN in cancer care.

E N D
ParenteralNutrition in CancerPatients Dr. Osman Abbasoğlu Professor of Surgery, Hacettepe UniversityDepartment of Surgery, Ankara December 8, 2018, İstanbul
Outline 1. Essentials of parenteral nutrition (PN) 2. Parenteral nutrition in cancer 3. Personal experience, conclusion
Outline 1. Essentials of parenteral nutrition (PN) 2. Parenteral nutrition in cancer 3. Personal experience, conclusion
2000; 59:457‒466 Parenteral Nutrition in the Critically-Ill Patient: More Harm than Good?
Is EN Really Safer Than PN? 0.57§ 0.72 “No significant difference in 30-day mortality associated with the route of delivery of early nutritional support in critically ill adults” No significant differences in the numberof treated infectious complications Harvey S.N Engl J Med. 2014;371:1673-1684.
PN Is as Safe as EN “Early nutritional support through the parenteral route, as it is typically administered, is neither more harmful nor more beneficial than such support through the enteral route” Harvey S. N Engl J Med. 2014;371:1673.
When Is ParenteralNutritionUsed? Patient Nutrition Assessment Functional GI Tract Parenteral Nutrition No Yes Short Term or No Central Access Long Term Enteral Nutrition Peripheral PN Central PN GIS Function Returns Yes No 8
Outline 1. Essentials of parenteral nutrition (PN) 2. Parenteral nutrition in cancer 4. Personal experience, conclusion
FrequentProblems in OncologyPatients • Intestinalfailure, peritonealcarcinomatosis • Severe mucositis • Severe diarrhea • Intractablevomiting • ……. Expectedsurvival >2 month
If the GIS is not functional, nutrition support can be given only by parenteral nutrition Intestinalobstruction Peritoneal carcinomatosis Intra-abdominal infections Ukleja A, et al. NutrClinPract 2010;25:403–14 Nehra V et al. J Nutr Biochem 1999;10:2-7
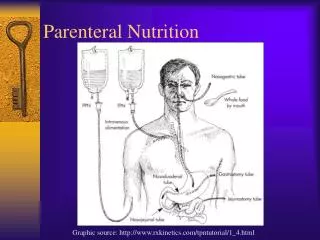
Ways of DeliveringParenteralNutrition Central PN • Right subclavian vein can be used as an access of choice • Tunneled catheters and implanted ports for long-term use Peripheral PN • Avoids morbidity related to central venous catheterization • Short-term (<2 weeks) therapy with low osmolar solutions
Role of PN: GastrointestinalDysmotility in CancerPatients GI dysmotility in surgicalpatients is common - Peritonealcarcinomatosis - Adverseeffect of medications - Intra-abdominalinfections - …. Nutritionalgoals can not be achieved Tube feeding with trophic EN Weimann A,Curr Opinion Crit Care.2016;19:353
Role of PN: GastrointestinalDysmotility in SurgicalPatients TrophicEN is veryimportant but allnutritionalrequirements can not be suppliedbytrophicnutrition Pharmacologicaloptionstostimulatebowelmotilityarelimited SupplementalParenteralNutrition Weimann A,Curr Opinion Crit Care.2016;19:353
Requirementsfor PN in Cancer • Glucose: 60%-70% • Lipids: 30%-40% Energy: 25-30 Kcal/kg/day • Usually 1.5 g/kg/day • Inceased demands in severe illness, injury, etc. Protein: At least 1 g/kg/day Vitamins, Trace Elements Water and Electrolytes Volkert D. ClinNutr, 2018
Most of thecomplications of PN are preventable! • Catheter insertion and catheter care standards • Avoidoverfeeding (increasesinfectionsandmortality) • Close monitoring of thepatients (avoidhyperglycemia) Pittiruti M . ClinNutr 2009;28:365 Cotogni P. JPEN 2013;37:375
Pathogenesis of Catheter Associated BSIs Contaminationof the Catheter or Catheter Hub (>10 Days) 2. Contamination of the IV Fluid (Rarely) 4. Migration of Skin Organisms (<7 Days) 1. SKIN FIBRIN SHEATH, THROMBUS VEIN 3. Hematogenous Spread (Less Commonly) Crnich CJ, Maki DG. Clin Infect Dis. 2002;34:1232
Pathogenesis of Catheter Associated BSIs Contaminationof the Catheter or Catheter Hub (>10 Days) 2. Contamination of the IV Fluid (Rarely) 4. Vastmajorityof central-line associated BSIs are preventable with the implementation of evidence-based interventions Migration of Skin Organisms (<7 Days) 1. SKIN FIBRIN SHEATH, THROMBUS VEIN 3. Hematogenous Spread (Less Commonly) Crnich CJ, Maki DG. Clin Infect Dis. 2002;34:1232
Supporting PN Safety PN prescribing, compounding, and dispensing and administration is a multidisciplinary process involving healthcare professionals representing the disciplines of: • Medicine • Dietetics • Nursing • Pharmacy in a Nutrition Support Team Trujillo EB. JPEN. 1999;23:109 2. Newton R. Nutrition. 2001;17:347 3. Saalwachter AR.Am Surg. 2004;70:1107
End of Life Care • Both EN and PN should be regarded as a medical treatment rather than a basic care • When the patient is close to the end of life, artificial nutrition is futile and unnecessary Orrevall Y. Nutrition 2015;31:610
Outline 1. Essentials of parenteral nutrition (PN) 2. Parenteral nutrition in cancer 3. Personal experience, conclusion
Experience at Hacettepe University BetweenJanuary 2015-December 2017 n Peripheral PN 811 Central PN 512 Total 1323
Complications of EN and PN are similar, 2017 data *p<0.05 Nutritionalgoals can be achievedwith SPN Kelleci B et al. 2018 40th ESPEN Congress Poster Presentation
Conclusions • Incancerpatients, if GI tract is not functional PN is thetreatment of choicefornutritionalsupport • If enteral nutrition alone is not able to provide the necessary nutrients, combination of EN with PN should be considered • PN is ususallysafeandmost of thecomplications can be preventedwithclosemonitoring