Download

1 / 32
400 likes | 1.17k Vues
Parenteral Nutrition. Made simple…. in 15 minutes Jon Shaffer Intestinal Failure Unit Hope Hospital. Parenteral nutrition. Importance of malnutrition Nutrition assessment Nutrition teams Indications Access Prescribing Monitoring. Parenteral nutrition. Importance of malnutrition

E N D
Parenteral Nutrition Made simple…. in 15 minutes Jon Shaffer Intestinal Failure Unit Hope Hospital
Parenteral nutrition • Importance of malnutrition • Nutrition assessment • Nutrition teams • Indications • Access • Prescribing • Monitoring
Parenteral nutrition • Importance of malnutrition • Nutrition assessment • Nutrition teams • Indications • Access • Prescribing • Monitoring
CONSEQUENCES OF MALNUTRITION DIMINSHED QUALITY OF LIFE INCREASED CLINICAL COMPLICATIONS POORER OUTCOME INCREASED COSTS
Malnutrition on admission –Sweden 382 pts • Infection • Surgery • Internal medicine • Oncology • Well nourished 73 % • Moderately malnourished 20 % • Severely malnourished 7 %
Parenteral nutrition • Importance of malnutrition • Nutrition assessment • Nutrition teams • Indications • Access • Prescribing • Monitoring
Nutritional assessment • Problem • No “blood urea “ for malnutrition • Risk scores v malnutrition • Multiple examples • Lack of a Gold Standard • Validation
Nutritional screening • ALBUMIN • Long half life • Overly sensitive- liver/renal disease • Reduction – redistribution • Slow to react with recovery • “ negative acute phase protein”
Nutritional screening • Subjective Global Assessment • Pt questionse.g weight loss • diet changes • GI symptoms • Physical appearance- • loss of fat • muscle wasting • Grading • A Well nourished • B Moderately malnourished • C Severely malnourished • Detsky 1987
Parenteral nutrition • Importance of malnutrition • Nutrition assessment • Nutrition teams • Indications • Access • Prescribing • Monitoring
Nutrition support teams • Appropriate screening /referral • Appropriate nutrition support • Education/training – staff and pts • Cost effective • PN x10 v EN • Better outcomes • Reduced complications • Bowling 2002
Efficacy of nutrition support teamse.g. catheter sepsis rates
Parenteral nutrition • Importance of malnutrition • Nutrition assessment • Nutrition teams • Indications • Access • Prescribing • Monitoring
Appropriateness – varies • Few ABSOLUTE indications • 1. Intestinal Failure • 2. If the gut works – use it • 3. Enteral preferable
If the gut works……1 • Technology -- 1970’s—1990 • Parenteral > Enteral • Better catheters/ better feeds/better research • Industry/ Surgery driven • Most - Surgical/Intensive care/Cancer
If the gut works……2 • 1990’s • Enteral tubes especially PEG’s • Medical > Surgical • Erosion of traditional markets e.g. Pancreatitis, ICU
Enteral ? preferable • Simpler • Less complications • Cheaper • Equieffective
Parenteral nutrition • Importance of malnutrition • Nutrition assessment • Nutrition teams • Indications • Access • Prescribing • Monitoring
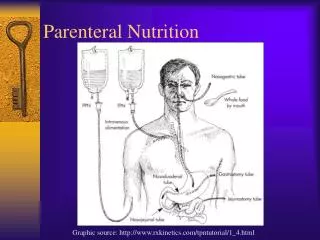
IV ACCESS • Peripheral - short term • Midline - short/medium • PICC ( Peripherally inserted central line ) -medium • Central – medium/long term • Central tunnelled – ultra long term HPN
Prescribing • Standard bags • A la carte • All in one bags • Re-feeding syndrome Po4, K
Design of Regimen • Osmolality peripheral < 900 mosmol/L, (1800kcals) PICC < 1200 mosmol/L (2000kcals) Central < 1700 mosmol/L (> 2000kcals)
Fluid • 30-35mls/kg body weight (adjust for age)
Energy • Normal to provide a ratio of • Glucose: fat 50:50 or 60:40 • Overfeeding can result in lipogenesis, fatty infiltration of the liver
Nitrogen • Range from 0.17-0.3gN/kg • Rarely give >14g / day • Need to ensure maximal metabolic effect of protein – 200kcals / gN • I.e. excess nitrogen = extra calories
Vitamins and Minerals • Water soluble • Fat Soluble • Trace Elements
Requirements • Energy = 8.1x45+656 =1020 + (153kcals)15% activity + (153kcals) 15 % stress + 500kcals = 1826kcals • Nitrogen = 0.2g/kg = 9gN • Fluid = 4 L (35mls/kg (1575mls) + losses 2.5L) • Na 295mmol (1mmol / kg, GI losses 250mmol/L) • K 45mmol (1mmol / kg) • PO 22.5mmol (0.5-0.7mmol/kg) • Mg 4.5mmol (0.1-0.2mmol/kg) • Ca 4.5mmol (0.1-0.2mmol/kg)
BAPEN British Association Enteral & Parenteral Nutrition