Mid-Altitude Training
Mid-Altitude Training. Power Available and Rate of Climb. Power output of non-turbocharged engines decreases ~2.5% per 1000’ climbed. ROC depends on excess power available, so it also drops with altitude. Do not attempt high ROC’s above 8,000’


Mid-Altitude Training
E N D
Presentation Transcript
Power Available and Rate of Climb • Power output of non-turbocharged engines decreases ~2.5% per 1000’ climbed. • ROC depends on excess power available, so it also drops with altitude. • Do not attempt high ROC’s above 8,000’ • Be particularly careful if AP is engaged in VS mode • VS attainable at low altitude may be impossible as altitude is gained • AP will attempt to maintain selected VS and will fly aircraft into a stall. • Recommend no more than 500 FPM selected above 8,000’
Relationship between IAS and TAS • The IAS attainable by an airplane is mostly a function of available power, which decreases with altitude. • At 17,500’ an SR-22 may cruise at 160 KTAS, with an IAS of only 120. • The way an aircraft handles and “feels” is mostly related to IAS, not TAS. • A given control deflection will be less effective; airplane may feel more mushy. • Autopilot will be less precise in control of aircraft
Icing • Even in summer icing is a concern above 10,000’: • Standard temperature lapse rate is 2C/ 1000’ • Takeoff from SL @ 20C, temperature at 10,000’ is approaching zero • Lifting present in summer cumulous can cause formation of Supercooled Large Droplets (SLD)- responsible for most severe icing possible. • At high altitudes: • Less power is available to counteract drag of ice • Margin between Stall IAS and Cruise IAS is smaller- increases chance of ice-induced stall • Do not fly into clouds if OAT is at or below 0C, regardless of season.
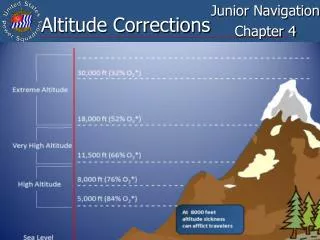
Atmosphere • Air is 78% Nitrogen, 21% Oxygen, 1% Other • Ratio stays the same as altitude increases, but density decreases • Atmosphere is half as dense at 18,000’ as at sea level.
Hypoxia • A lack of sufficient oxygen in cells and tissue caused by: • Inadequate supply of oxygen • Inadequate transportation of oxygen • Inability of the body tissues to use oxygen
Types of Hypoxia • Hypoxic • Caused by insufficient oxygen in inhaled air • Histoxic • Inability of cells to use oxygen • Caused by alcohol or drugs • Hypemic (Anemic) • Reduced oxygen carrying capability of blood • Carbon Monoxide/ Tobacco Smoke reduced ability of blood to transport oxygen • Smoker’s apparent altitude at SL is ~7,000’ • Stagnant • Reduced circulation of blood to tissues • Coronary Artery Disease • Excessive G-Forces
Hypoxia- Potential Symptoms • Impairment of: • Judgment • Memory • Alertness • Coordination • Ability to make calculations • Headache • Drowsiness or fatigue • Dizziness • Increased breathing rate • Sweating • Euphoria or belligerence • Loss of peripheral vision • A blue coloration of the fingernails and lips • Tingling or warm sensations
Factors Exacerbating Hypoxia • Inhaling carbon monoxide • Cigarettes • Exhaust fumes • Anemia • Genetic • Pregnancy • Medications/ Drugs • Alcohol • Antihistamines • Tranquilizers • Sedatives • Analgesics (pain-killers) • Extreme heat and cold • Fever • Anxiety
Decompression Sickness • Two Forms: • Trapped Gas • Expanding or contracting gas in body cavities during altitude changes can result in abdominal pain, toothache, or pain in ears and sinuses if the person is unable to equalize the pressure changes. • Above 25,000’ distention can produce particularly severe gastrointestinal pain. • Evolved Gas • Air we breath is 78% Nitrogen. • Most nitrogen is exhaled from the lungs; some is absorbed by the body. Absorbed nitrogen does not normally present problems because it is carried in a liquid state. • If ambient pressure lowers drastically, absorbed nitrogen changes from a liquid to a gas in the form of bubbles which can have adverse effects on some body tissues. • Fatty tissue contains more nitrogen than other tissue; thus making overweight people more susceptible to evolved gas decompression sicknesses.
Decompression Sickness • Types of evolved gas decompression sickness: • The bends (Caisson disease) • Characterized by pain in and around the joints. • Pain gradually becomes more severe, can become temporarily incapacitating, can result in collapse. • “The chokes” • Chest pains and burning sensations • A desire to cough • Cyanosis • Sensation of suffocation • Progressively shallower breathing • Ultimately, collapse and unconsciousness. • Paresthesia (“Pins and Needles”) • Tingling and/ or itching • A red rash • Cold and warm sensations • Shock can result from decompression sicknesses as a form of body protest to disrupted circulation, can cause: • Nausea • Fainting or dizziness • Sweating • Loss of consciousness. • The best treatment for decompression sickness is descent to a lower altitude and landing. If conditions persist after landing, recompression chambers can be located through an aviation medical examiner.
SCUBA • Diving will compound decompression sickness due to compressed air breathed during dive. • After diving, flying to 8,000’ exposes a person to the same effects as a non-diver flying unpressurized at 40,000’. • FAA recommendation and ASE policy on waiting periods is: • After decompression stop dive, at least 24 hours. • After non-decompression stop dive: • If flying above 8000’, at least 24 hours. • If flying at or below 8000’, at least 12 hours.
Vision at Altitude • Reversal of light distribution at high altitudes (bright clouds below the airplane and darker, blue sky above) can cause a glare inside the cockpit. • Glare effects and deteriorated vision are enhanced at night when the body becomes more susceptible to hypoxia and can occur at altitudes as low as 5,000 feet. • Empty visual field caused by cloudless, blue skies during the day can cause inaccuracies when judging the speed, size, and distance of other aircraft. • Sun's ultraviolet rays at high altitudes are more intense- sunglasses are recommended.
Negative Effects of Oxygen • Prolonged use can be harmful to health, with symptoms including: • Bronchial cough • Fever • Vomiting • Nervousness • Irregular heart beat • Lowered energy • Symptoms appeared on the second day of breathing 90 percent oxygen during controlled experiments. It is unlikely that oxygen would be used long enough to produce the most severe of these symptoms in any aviation incidence. • Prolonged flights at high altitudes using a high concentration of oxygen can produce some symptoms of oxygen poisoning such as infection or bronchial irritation. • Sudden supply of pure oxygen following a decompression can often aggravate the symptoms of hypoxia. • Oxygen should be taken gradually, particularly when the body is already suffering from lack of oxygen, to build up the supply in small doses. • If symptoms of oxygen poisoning develop, high concentrations of oxygen should be avoided until the symptoms completely disappear.
Regulations re: Oxygen Use • Flight Crew must use oxygen at Pressure Altitudes: • Above 14,000’ for any time • 12,501’- 14,000’ for more than 30 min • All passengers must be provided with oxygen above 15,000’ PA • Flight Crew must use oxygen at PA- • Above 12,000’ for any time • 10,001’-12,000 for more than 30 min FAR’s ASE P+P’s
Dual-Lumen Cannula* Face Mask Oxymizer Cannula PreciseFlow* A3 Flow Meter Oxygen System Components Cannula/ Mask Only in Emergency Regulator Oxygen Tank *Preferred Equipment
Outlet to Regulator MasterOn/ OffValve Pressure/ (Quantity)Gauge Oxygen Bottle
02fromtank Outlets ModeSelector AltitudeSelector PreciseFlow Demand Conserver • Regulates 02 to mask so that 02 only flows when wearer is breathing • Useable with dual-lumen cannula or mask • With cannula: • Connect “Delivery” and “Sensing” outlets to cannula • Set mode selector to “CONSERVE” • With mask: • Connect “Delivery” outlet to mask • Set mode selector to “CONSTANT” • Set cruise altitude against triangle with altitude selector • Flow indicator built into tubing from 02 tank • Shows on/ off only, not rate of flow
FlowIndicator AltitudeScale FlowControl A-3 Flow Meter • Hold vertically, adjust flow until floating ball (flow indicator) is at level of cruise alt on alt scale • Check every 15 min with pulse oximeter check • Normally use only with Oxymizer cannula • In case of nasal blockage/ equipment malfunction, may use with mask: • With mask, adjust flow to maximum (full open), regardless of altitude
Worn inNose ToPreciseFlow Dual- Lumen Cannula • Use only with PreciseFlow regulator • Worn in nose: • Only effective when breathing nasally • Talking, mouth breathing reduce effectiveness and lower Sp02 • Limitations: • Face mask must be accessible for anyone required to use/ have available O2, in case nasal blockage develops • May not be used above 18,000’ • Regular smokers may not get enough oxygen with cannulas: • Add 7,000’ to cruise altitude when adjusting flow • Not recommended above 11,000’
ToA-3 FlowMeter Worn inNose Oxymizer Cannula • Use only with A-3 flow meter • Bladder holds O2 until breathed in; allows for lower flow rate than mask • Same concerns and limitations as dual-lumen cannula
ToRegulator Face Mask • Normally use only with PreciseFlow regulator • May use with A-3 if cannula malfunctions or is ineffective • Use: • If nasal blockage experienced • Smoker who needs high flow rate • Not guaranteed to work with beard • Higher the altitude, worse the effectiveness with beard • Need to use hand mike when wearing • Push boom mike up
Oxygen System- Preflight Inspection • Visual inspection of: • Masks, cannulas, and tubing for tears, cracks, or deterioration • Regulator for valve and selector condition and positions • Oxygen quantity • Don mask or cannula and perform functional check of flow, flow indicators, and connections. • Verify that all components and valves are shut off.
Oxygen System- General Tips • Unless aircraft is full, always have one more regulator and mask/ cannula set up and connected than required • Don cannula or mask before TO if planning a climb to >10,000’, easier than donning in-flight • Immediately prior to takeoff: • Turn on O2 at bottle • Turn regulator to high flow level and verify flow • Turn off regulator until O2 needed • Petroleum products, such as lipstick, chapstick, and hair oil may spontaneously combust in the presence of 100% O2 • Do not use, and ensure that passengers do not use, if using O2 • No occupants may remain in the aircraft if O2 bottle is refilled while in aircraft • Anecdotal evidence suggests women: • May need O2 earlier than men • May need to set flow to higher than cruise alt.
Worn with fingernail against screen side, turns on automatically when worn. Artificial fingernails may impede reading Nail polish said to be OK Uses red and infrared light to measure pulse rate and level of oxygen saturation in blood (SpO2). ASE Policy is to check SpO2 every 15 minutes when using oxygen, or with any concern re: hypoxia. Maintain SpO2 above 90% If necessary adjust O2 flow to higher altitude than cruise altitude. Pulse Oximeter (Green, Yellow, or Red)
Pulse Oximeter- Limitations • Does not detect nor account for effect of carbon monoxide in blood: • Doesn’t warn about CO poisoning • Smokers’ SpO2 may look fine even when hypoxic • Dependent upon presence of a good pulse; may not get good reading with: • Very low blood pressure • Impaired blood flow to the fingers • Cold temperature causing constriction of the blood vessels in the extremities • Drug use which causes: • Vasoconstriction or vasodilation (e.g., nitroglycerine), or • Change in blood color (e.g., sulfonamides).
Oxygen System Failure • If no or low flow is suspected, check: • Connections: • Tank to regulator (likely to pop off) • Regulator to mask • Kinks or twists in lines • Master on/ off valve • Flow adjustment on regulator • Try another mask/ cannula and regulator hook-up • If unable to resolve quickly, descend to 10,000’ or lower
Emergency Descent 1. Power Lever- IDLE 2. Mixture- AS REQUIRED • Caution • If significant turbulence is expected do not descend at indicated airspeeds greater than VNO (178 KIAS) 3. Airspeed- VNE (201 KIAS)