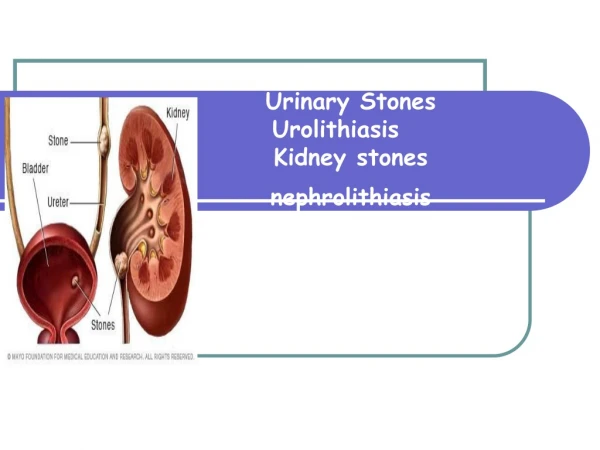
Urinary Stones
Urinary Stones. Epidemiology Pathology of stones Types of stones Physiochemistry of stone formation Factors which predispose to recurrent stones Medical Anatomical Drugs Assesment of recurrent stone formers General and Specific Medical Management Alpha-blockers. Epidemiology.

Urinary Stones
E N D
Presentation Transcript
Urinary Stones • Epidemiology • Pathology of stones • Types of stones • Physiochemistry of stone formation • Factors which predispose to recurrent stones • Medical • Anatomical • Drugs • Assesment of recurrent stone formers • General and Specific Medical Management • Alpha-blockers
Epidemiology • Prevalance in US – 10-15% • Prevalence in South Australia 6-7% • General Risk factors • Age/Gender/Race – 40-60 y/o males, whites>hispanics>asian>african americans • Geography – 'Stone belts' • Dry, hot areas or tropical areas • Factors – dehydration (Curhan), lots of sunlight (vitamin D), water hardness not found to be a factor • Occupation – cooks/boiler workers • Dehydration/heat exposure • Obesity – Curhan – increased insulin levels and syndrome X – hypercalciuria and hyperuricouria
Pathology of renal stones - Types • Calcium • Oxalate – 60% • Monohydrate – hourglass, Dihydrate – envelope • Hydroxyapatite – 20% • Amporphous • Hydrogen Phosphate (Brushite) – 2% • Needles • Non Calcium • Uric acid – 7% • Amorphous • Struvite (Magnesium Ammonium Phophate) – 7% • Coffin Shaped • Cystine – 1% • Hexagonal • Other – indinavir, triamterene, silica, adenine, etc. • Mineral & Non-mineral component
Physiochemistry of stones • Saturation Theory, Nucleation and Retention • Substances Precipitate (Saturation) • Stones form due to supersaturation • Ksp = Thermodynamic solubility product (Concentration at which saturation is reached and cystallization occurs) • 3 levels of saturation • Undersaturated • Metastable – heterogenous nucleation occurs but homogenous nucleation slow • Unstable – can get homogenous nucleation • Crystals are formed (nucleation) • Crystals are retained (Retention) • Fixed particle theory – adherence to renal epithelium via substances including osteopontin, hyalurin • Free particle theory – issues re: transit time
Physiochem (2) • Inhibitors & Promoters • Can act on variety of stages of crystal development • precipitation, nucleation, growth • Ksp is calculated in water, tend to get precipitation in urine when Ksp exceeded by 7-10 times • Inhibitors • Apply to CaOx and CaPO4 stones (no inhibitors for uric acid stones) • Urinary glycoproteins – nephrocalcin, Tamm-Horsfall protein, osteopontin • Citrate – binds free calcium therefore amount for precipitation is decreased
Physiochem (3) • Promoters • Low urine volume • Increased concentration of solutes • Urinary stasis – many conditions which produce stasis eg. MSK, calyceal diverticula, PUJ, Horseshoe, etc are aslo associated with underlying metabolic abnormalities • Matrix • Non Crystalline organic component of stones • Unknown role in stone formation • Forms 2-5% of Ca stones, 65% of struvite stones • Randall's Plaques – calcium salt deposits on papillae • Associated with recurrent calcium stones • Increased surface area of RP associated with decreased volume & pH, increased urinary calcium • Recurrent stone former kidneys histology – found stones attached to plaques
Predisposing Factors to stones (Mad) • Medical – related to type of stone • Calcium • Hypercalciuria • Hyperoxalouria • Hyperuricouria, low pH, low volume • Hypocitraturia and hypoMg • RTA • Uric acid stones • Low pH, hyperuricouria, low volume • Cystine - Cystinuria • Struvite – Proteus & other infections • Other – Xanthine, adenine, ammonium uric acid
Predisposing Factors M – Ca (1) • Hypercalciuria • Most common metabolic abnormality found in recurrent stone formers (35-65%) • Treatment of hypercalciuria – decreases recurrence • Link with Randall's plaques • Definition • >200mg/day of urinary calcium after a 400mg/day Ca and 100mg/day Na diet for a week • >4mg/kg/day (7mmol/day men, 6mmol/day women)
Predisposing factors M (Ca 2) • Hypercalciuria • Absorptive (40%), resorptive (5%), renal (10%) • Absorptive • >0.2mg of Ca/mg of creatinine after an oral calcium load • Has a normal PTH and usually normocalcaemia • Type I – Does not normalise despite a restricted Ca diet of 400mg/day for a week • Type II – Normalises with a restricted Ca diet • Pathophysiology – increased intestinal absorption of calcium • Transient rise in serum Ca, PTH down, urinary Ca increased • Unknown cause
Predisposing factors M (Ca 3) • Renal Hypercalciuria • Due to impaired resorption of calcium • Associated with normocalcaemia, PTH increased • Unknown cause • Pathophys – impaired resorption of calcium • PTH increases to try compensate for the loss of Ca • Vit D & osteoclasts up • Overall serum Ca normal due to bone & intestinal resorption increased
Predisposing Factors M (Ca 4) • Resorptive Hypercalciuria • Due to primary hyperparathyroidism • PTH and serum Ca increased (vs other forms of hypercalciuria) • Cause - >90% - solitary parathyroid adenoma • Multiple parathyroid adenoma/hyperplasia • Parathyroid carcinoma • Needs neck U/S , sestamibi scan • Other causes of hypercalciuria • Sarcoid/TB/Histoplasma – due to Vit D increased • Malignancy (lung,breast,renal,myeloma) – due to mechanical bony destruction, hormonal bony destruction (PTHrP, IL-1, TNF-alpha) • Steroids – PTH increased, but intestinal resorption decreased
Predisposing Factors M (Ox1) • Hyperoxalouria • >40mg/day urinary oxalate • Causes stones via – saturation theory & retention fixed particle theory • Primary & Dietary, Idiopathic, Enteric • Primary – AR recessive disorder of glycine metabolism (80% urinary oxalate endogenous glycine & ascorbic acid metabolism) • Urinary oxalate >100mg/day • Type I – alanine glyoxylate aminotransferase, Type II gloxylate reductase • Rarely seen in adults – causes renal failure by age 15 y/o, liver/kidney transplant • Dietary • High oxalate (nuts, chocolate, spinach), high oxalate precursors (vitamin C, glycine), low chelators (Ca & Mg decreased either due to dietary lack or excess other chelators eg tetracyclines)
Predisposing Factors M (Ox2) • Hyperoxalouria • Enteric – Most common cause • Due to malabsorption – lack of chelators & increased permeability of colon to oxalate, loss electrolytes, H+, fluid) • Causes – short gut, jejunalileal bypass, chronic diarrhoea, obesity surgery, IBD, Coeliac • Associations • low urine pH & volume • Hypocitraturia & hypoMg • Hypokalaemia
Predisposing Factors M (U1) • Hyperuricouria - >600mg/day • Effect – decreased effectiveness of Calcium stone inhibitors (GAG and heparin) • PH <5.5 – pure uric acid stones • PH >5.5 – mixed Ca and uric acid stones (heterogenous) • Causes – dietary & increased cell turnover (myeloproliferative, cytotoxics, haemolytic anaemia) • Gouty diathesis • Stone formation with low pH +/- gouty arthritis • Associated with chronic metabolic acidodis & hypocitraturia
Predisposing Factors M (citrate) • Hypocitraturia - <320mg/day • 2nd most common metabolic abnormality in Ca stones (after hypercalciuria) • Due to metabolic acidosis which causes • Increased tubular resorption of citrate • Decreased tubular synthesis • SNR, IP • 4 causes of hypocitraturia • Chronic diarrhoea • RTA • Idopathic, excess dietary protein • Drugs – thiazide, enalapril
Predisposing Factors M (RTA) • Metabolic acidosis due to impaired renal handling of H+ or HCO3 • Type I – impaired H+ excretion • Type II – impaired HCO3 resorption • Type IV – chronic renal failure • Type II & IV not normally associated with stones (Type II – proximal RTA, normal citrate levels, Type IV – CRF - can't excrete enough substrate to get saturation)
Predisposing factors – M (RTA 2) • Type I RTA • Most common form of RTA • 50-70% of patients with type I RTA have stones due to hypocitraturia • Defect in DCT K+/H+ ATPase – imparied H+ excretion – metabolic acidosis • Associations – hypokalaemia, hyperchloraemia, urine pH >6, nephrolithiasis, nephrocalcinosis (hyperparathroidism, MSK, type I RTA) • The metabolic acidosis causes increased bone resorption (hypercalciuria) & hypocitraturia • Most common stone is Calcium Phosphate (urinary pH high, hypocitraturia, hpercalciuria)
Predisposing factors – Cystine • AR disorder associated with impaired transport of COLA dibasic aminoacids • Causes stones due to cystinuria - >300mg/day urinary cystine, associated with hypercalciuira, hyperuricouria, hypocitraturia • AR, chromosome 2 & 19 • Type A – 2, Type B – 19, Type AB – 2 & 19 • Clin – recurrent stones in childhood (causes 10% of stones in kids, 1 stone event every 1-2 years), bilateral recurrent stones (cystine and calcium) • Associated with hypotonia, Fanconi's syndrome
Predisposing factors – cystine 2 • Cystine stones formation is related to saturation theory – concentration of cystine and the pH • Therefore try reduce cystine excretion to less than 300mg/L – Medical Mx • Fluids – 3L urine output/day, citrus products • Want specific gravity <1.01 • PH – small pH window to aim for • Cystine does not solubilise until pH>7.5 • Calcium PO4 stones occur when pH >7.5 • Aim for pH 6.5-7 with K citrate or NaHCO3 • Drugs – penicillamine, D-mercaptopurine, thiola, captopril – try to break disulfide bond in cystine
Predisposing factors Cystine 3 • Surveillance – 3-6/12 U/S, monitor urine pH, specific gravity and cystine excretion • Proactive stone removal • Try to keep it minimally invasive • ESWL resistant (esp S subtype of stones)
Predisposing factors - struvite • MAP hexahydrate (coffin shaped) • Only occur with urea-splitting bugs • Proteus (esp miribalis & vulgaris) • Klebs, Pseudomonas, Staph • Not E coli • Cause stones via mucousal damage (fixed particle) • Urease – • get lots of HCO3 and ammonium • alkalinizes urine • phophate buffer disassociates – PO4 high • + Physiologic Mg • Get full house of Mg Ammonium Phosphate
Predisposing factors -drugs • Direct precipitation • Indinavir – protease inhibitor, high renal clearance, low solubility. CT invisible. • Triamterene – K+ sparing diuretic. Incorporated into rather than forms stones • Silicate – from anatacids • Ephedrine • Indirect • Diuretics • thiazide – intracellular acidosis & hypoC • Frusemide – hypercalciuria • Acetazolamide – metabolic acidosis & hypoC • Laxatives, cytotoxics, corticosteroids&vitD
Predisposing factors - Anatomical • Get stones due to obstruction & associated metabolic abnormality • Kidney • MSK – ectasia of renal collecting ducts, 1/5000, 10% develop problems due to infection/stones, associated with hypercalciuria and hypocitraturia • Horseshoe – Median fusion of metanephric tissue with entrapment of IMA and malrotation, 1/500. Issues – stones, infection, PUJ obstruction, metabolic abnormalities • Caliceal diverticulum – Non-secretory outpouching of renal collecting system. 1/500. Assoc with hyperCa, hyperOx, hyperU, low pH, hypo C • Ureter – PUJ, reflux, strictures, ureterocoele
Metabolic workup of people with stones • Baseline recurrence risk in adult, calcium stone, first episode, no risk factors is 50% at 10 years • Who to investigate? • Anyone with a stone who wants a metabolic work up? • Risks – economics, compliance, often normal metabolic work up • Calcium stone formers – recurrent, multiple • Uric acid/Cystine stone formers • Associated medical conditions – bone/GI/nephrocalcinosis/gout, GU anatomic abnormalities • Children • People who can't risk multiple stone attacks • Solitary kidney, infirm, difficult to manage stones
Abbreviated protocol • History & Exam – MAD • Bloods – NA, K Cl, urea, Creatinine, Ca, uric acid, PTH • Urine – pH, MCS, Stone analysis • Xrays - ?presence of anatomic abnormalities
Full metabolic work up • Variety of protocols involving one to three 24 hour urine collection (Creatinine, Na, pH, volume, oxalate, citrate, uric acid) • +/- fast and load calcium testing to help differentiate between the various causes of hypercalciuria • Adequacy of the 24 hour collection • Assess the creatinine content – males – 15-20mg of creatinine/kg, females 10-15mg of creatinine/kg in 24 hour period (depends on body composition) • Use laboratory supplied container • Discard the initial 1st void urine and then collect all samples for a 24 hour period and keep the final 1st void urine of the next day
General Medical Management • Fluid, Sodium, Protein, Calcium, Oxalate, Obesity • Fluids • Volume – want at least 2L of urine /day – Borghi • Water hardness – no clinical effect on stone formation • Carbonated beverages – may improve stone recurrence rates (only if Citric acid vs Phosphoric acid) • Citrus – Citrate is metabolized to HCO3. The accompanying anion is important – Orange juice and grapefruit have K+ (good), cranberry has H+ (bad) • Sodium • High salt intake causes hypercalciuria (like frusemide) • Hypocitraturia (via Na induced HCO3 loss – acidosis) • Increases saturation of urine urate • Reduces effect of thiazides • Try limit salt to 2000-3000mg /day
General Medical Management • Protein • The amino acids cause an acid load • urine pH drops • urinary citrate drops • urinary calcium increases (due to increased bone resorption and reduced renal resorption) • Uric acid and oxalate levels also rise • Atkins diet – lead to lower urine pH, hypocitraturia, hypercalciuria and hyperuricosuria – stones • Generally try reduce the protein intake (2 serves/day) • Oxalate • Only 15% of urinary oxalate from dietary sources • Try avoid excess vitamin C (<2g/day)
General Medical Management • Calcium • Excess restriction leads to increased oxalate absorption (lack of chelators) and other complications • Take calcium supplementation with meals (to bind the oxalate from the meal) • Calcium citrate better than calcium carbonate • Monitoring • Stay on the diet for 3-4 months then reassess the metabolic parameters • Long term compliance issues • Allows institution of specific medical Mx if the dietary measures are not working
Medical Therapy for Stone Passage • Stone size 5mm or less, position (distal better than proximal) associated with better rates of spontaneous passage (usually takes 30-40 days from onset of symptoms) • Alpha blockers and Calcium channel blockers have been shown to reduce time to passage and improve spontaneous passage rates • Lack of good RCT, esp given variations in stone size and position • Estimated ARR is about 65% in people given Calcium channel or alpha-blockers • Lancet, Vol 368. 2006 p 1171
Medical Management in Kids • Neonates • Frusemide induced nephrolithiasis • Cease frusemide, swap to thiazide, monitor for renal damage • Children and Adolescents • Higher risk of definable metabolic abnormalities • Esp cystinuria, RTA I, primary hyperoxalouria • Urol Clin N America 31 (2004) 575-587
Medical Management Pregnancy • Radiation in pregnancy – threshold risk of damage to foetus is 1.2 rad. • Plain xray (limited IVP) each image = 0.1-0.2 rad • Stones not visible on MRI (shows hydroureter well, can try differentiate from HUN of pregnancy) • Try to do the minimum possible to keep the kidney functional and patient asymptomatic until the baby is born • If stented – need to change every 4 weeks • Calcium supplementation in pregnancy – use calcium citrate rather than carbonate