Kidney Stones
Kidney Stones. Wael AlJaroudi, MD Editor: Amy Shaheen, MD, Assistant Professor of Clinical Medicine Duke University Medical Center. Epidemiology. Epidemiology Kidney stones (also called Nephrolithiasis or urolithiasis) are common health problems

Kidney Stones
E N D
Presentation Transcript
Kidney Stones Wael AlJaroudi, MD Editor: Amy Shaheen, MD, Assistant Professor of Clinical Medicine Duke University Medical Center
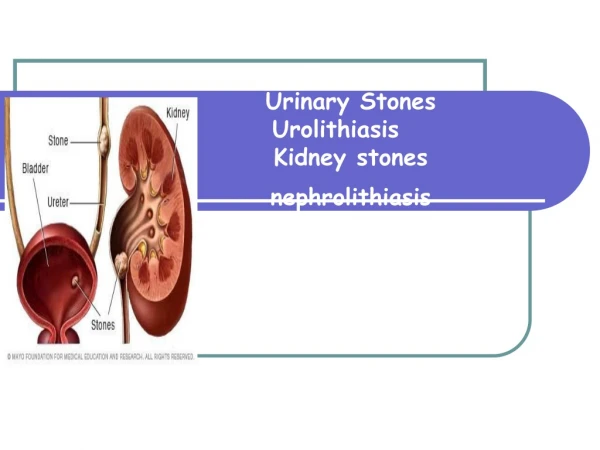
Epidemiology Epidemiology • Kidney stones (also called Nephrolithiasis or urolithiasis) are common health problems • The prevalence of stone-forming disease rose from 3.8 percent in the late 1970s to 5.2 percent in the late 1980s and early 1990s. • It is more common in men > women, white > African American • It is estimated that 12 % of men and 5 % of women will develop symptomatic kidney stones by the age of 70 • It has been estimated that for patients who have already had a stone, the likelihood of forming a second stone is about 15 percent at one year, 35 to 40 percent at 5 years, and 80 percent at 10 years.
Pathogenesis Pathogenesis For a stone to form, 3 processes occur: • Supersaturation: Cations and anions are charged soluble molecules such as calcium and oxalate. However, at a specific concentration and pH, the equilibrium state of these molecules reach a critical point called supersaturation. Beyond this point, these molecules cannot remain dissolved and will become insoluble and precipitate 2. Nidus: A nidus represents a focus where crystals start precipitating. 3. Aggregation: Aggregation is the process where precipitating crystals accumulate on each others and form a bigger crystal in a geometrical and organized fashion.
Type of kidney stones Type of kidney stones 1.Calcium stones account for 80 % of all kidney stones -Calcium oxalate (monohydrate and dihydrate) are the most common -Calcium phosphate 2.Uric acid stones 3.Struvite stones (composed of magnesium, ammonium, calcium and phosphate) 4.Cystine stones 5.Indinavir stones (limited to HIV-infected patients)
Calcium Stones Calcium stones -Calcium stones are the most common type of kidney stones -Citrate is the most powerful inhibitor of Calcium oxalate stone formation -Hyperoxaluria is the most important factor in the formation of calcium oxalate stone
Calcium Stones (cont.) -Calcium phosphate stones are the second most common calcium stones after calcium oxalate: they are more common in patients with distal RTA1, patients on acetozolamide ( alkaline pH which leads to CaPO4 precipitation). -Calcium stones precipitate in alkaline urine. -They are radio-opaque and are seen on xray films
Calcium stones: Risk factors Calcium stones: Risk factors: 1.Low fluid intake/ Low urine Volume: Increases the concentration of lithogenic factors in the urine. 2. Hypercalciuria: occurs with hypervitaminosis D, distal RTA 1, sarcoidosis, primary hyperpathyroidism, excessive calcium intake. 3. Hypocitraturia: Occurs in patients with RTA 1 or chronic metabolic acidosis. Citrate chelates calcium and prevent stone formation. Citrate is the most powerful inhibitor of calcium stone formation 4. Hyperuricosuria: Occurs with high protein intake resulting in high uric acid production/excretion. Uric acid act as a nidus for crystal formation 5. History of prior calcium stones
Calcium stones: Risk factors (cont.) Risk factors for calcium stones (continued) 6. Hyperoxaluria: Most important factor in calcium oxalate formation. It is present in mildly elevated amount in up to 40 percent of male and 15 percent of female stone formers. Marked hyperoxaluria is usually associated with inflammatory bowel disease and/or malabsorption: free bile acid chelates calcium in the GI tract allowing more oxalate absorption and hence urinary excretion.High Vit C consumption, ethylene glycol are also associated with hyperoxaluria 7. Medullary sponge kidney: Accounts for 10-20% of calcium stone formers 8. RTA type 1: It is associated with hypocitraturia and hypercalciuria and alkaline pH
Calcium stones: Risk factors (cont.) Risk factors for calcium stones (continued) 9. Primary hyperparathyroidism: Associated with hypercalciuria 10. Gout: associated with hyperuricosuria which acts as a nidus 11. HTN: associated with hyperuricosuria 12.High animal protein: results in high uric acid production and hence excretion 13. High NaCl intake: leads to increased urinary calcium excretion 14. Low calcium intake: Results in less oxalate chelation in the GI tract, more oxalate absorption and hence hyperoxaluria
Uric Acid Stone Uric Acid Stone: -Uric acid stones precipitate in acidic urine, mainly with a pH <5.5 -They are radiolucent and do not show on a regular xray film
Uric Acid Stone (cont.) Uric acid Stone Risk factors: 1.Hyperuricosuria - 10-20 % of gout patients overproduce uric acid leading to increased excretion -Inherited enzyme defects leading to purine overproduction (eg. Lych Nyhan syndrome) -Urate overproduction: (myeloproliferative disorders, obesity, lymphoma,hemolysis, glycogen storage disease, ethanol, vit b12 deficiency, chemotherapy..) 2. Chronic diarrhea: Results in bicarbonate loss, acidic concentrated urine which precipitates uric acid stone
Struvite Stones Struvite Stones -Struvite stones occur in patients with chronic urinary infections due to a urease producing organism -The urease enzyme splits urea into ammonium. -Ammonium binds with phosphorus, magnesium and calcium and form the struvite stone -Urease producing bacteria include proteus (most common), pseudomona, yeast, and Staph (PPYS = piss) -They are rapid forming and often cause staghorn calculi -They precipitate faster in alkaline urine -They are less radio-opaque then calcium stones
Cystine Stones Cystine Stones: -Cystine stones develop in patients with cystinuria, an autosomal recessif disease associated with increased excretion of cystine. -They tend to recur very frequently and often can cause urinary obstrcution and compromise kidney function -Heterozygote/carriers of the disease do not form stones -They precipitate faster in acidic urine
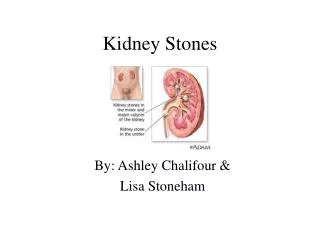
Clinical Symptoms • Clinical symptoms: -Kidney stones often are asymptomatic -Usually, the first symptom of a kidney stone is pain. Pain occurs when there is obstruction of the urinary tract and spasm. Pain is colicky, waxes on/off, sharp, often associated with nausea/vomiting. Its location varies with the location of the stone and can migrate to the suprapubic area and groin as the stone moves down the ureter. -Microscopic/macroscopic hematuria -Dysuria
Evaluation of Kidney stones Evaluation of kidney stones -Workup on initial kidney stone includes: calcium level (r/o hyperparathyroidism, hypervitaminosis D), phopsphorus, electrolytes such as bicarbonate (r/o RTA type 1), U/A with culture, and an imaging modality. Although IVP has been the standard, current data shows that CT renal protocol is as sensitive and specific and does not require contrast.
Evaluation of kidney stones Evaluation of kidney stones (continued) -Urinary pH. A pH >7 (alkaline) is usually associated with calcium phosphorus stones and struvite stones. A pH <5.5 (acidic) is usually associated with cystine and uric acid stones -Crystal morphology is helpful in determining the type of stone
Calcium oxalate crystals Calcium oxalate crystals:urine sediment shows envelop shape dihydrate stone (small arrow), and dumbbell shape monohydrate crystals (long arrow) which could also have a needle appearance.
Uric Acid Stone Uric acid stone: Urine sediment shows pleomorphic Rhombic plates or diamond shape crystals
Struvite Stone Struvite stone: Urine sediment shows “coffin lid” crystals
Cystine Crystal Cystine crystal: Urine sediment shows hexagnal Crystals which are pathognomonic of cystine stone
Recurrent kidney stones For recurrent kidney stones, additional work up includes checking for 24 hr urine volume, cystine, calcium, Na, citrate, urea, uric acid, and creatinine excretion. • Men: Calcium <300 (7.5 mmol/day)/ Female: <250 (6.25 mmol/day) Men: Uric acid <800 (4.8 mmol/day)/ Female: <750 (4.5 mmol/day) Men and Female: Oxalate <45 (0.5 mmol/day) • The standard lower limit of normal for citrate is 320 mg for men and women.
Imaging Modality • Imaging modality -IVP used to be the gold standard. -Non-contrast-enhanced helical CT scan has proven to be accurate in detecting of kidney stones -It is important to appreciate that ureteral dilatation without a stone on radiologic examination could represent recent passage of the stone - Renal ultrasonography is an alternative in pregnant women, but this cannot localize ureteral stones, which can often be detected by transvaginal ultrasonography
Imaging Modality (cont.) Imaging Modality: - The stone characteristics on CT scan may suggest the type of stone that is present: - Although magnesium ammonium phosphate and cystine stones are often radiopaque, they are not as dense as stones comprised of calcium oxalate or calcium phosphate. - Calcium phosphate stones are more likely found in the presence of nephrocalcinosis, which is suggestive of renal tubular acidosis. Bilateral calcifications at the corticomedullary junction is typically seen in medullary sponge kidney and in this setting calcium oxalate or calcium phosphate stones may be found - The presence of staghorn calculi favors struvite stones - Uric acid stones are radio-lucent on xray but visible on CT scan
Treatment • Treatment • Non obstructing stone Calcium stone: -Increase fluid intake to 2 L per day. Decrease dietary protein and Na. -If urinary calcium is elevated, evaluate for high Vit D, hyperparathyroidism and treat accordingly Thiazide diuretic decrease hypercalciuria -If hypocitraturia is present, supplement with potassium citrate. If the pH is >6, citrate supplementation should be avoided because of the increased pH alkalanization and higher risk of stone precipitation
Treatment (cont.) • Treatment • Medical management -If hyperoxaluria is present, the approach to intervention depends on the diet and the urine calcium. If the urine calcium is not high, increasing dietary calcium should be considered along with a low oxalate diet. Food with high oxalate content include: • beets rhubarb • chocolate spinach • coffee strawberries • cola tea • nuts wheat bran
Treatment: Medical Management (cont.) • Treatment • Medical management (continued) -If hyperuricosuria is present, lifestyle modification with the aim of reducing uric acid production (i.e. decreased purine intake and weight loss) should be implemented. However, if the urine pH is 6 or higher, the high urine uric acid may not be playing a role as it will stay in solution.Allopurinol can help decrease uric acid in patients who are overproducers. -Do not decrease calcium intake; this will increases oxaluria
Treatment: Medical Management (cont.) Medical management (continued) Uric acid stone -Allopurinol +/- urine alkalinization -Low purine diet -High fluid intake -Avoid urine alkalinization if there is superimposed hypercalciuria
Treatment: Medical Management (cont.) Medical management (continued) Struvite stone -Acidification of the urine -Antibiotics -Removal of the stone -If stones cannot be removed, acetohydroxamic acid (AHA) can be used with long-term antibiotic drugs to prevent the infection that leads to stone growth.
Treatment: Medical Management (cont.) Medical management (continued) Cystine stone -Increased fluid intake -Alkalinization of the urine -Penicillamine forms soluble complexes with cystine but not well tolerated
Surgical Treatment B. Surgical treatment -Surgery should be reserved as an option for cases where other approaches have failed. Surgery may be needed to remove a kidney stone if it: • does not pass after a reasonable period of time and causes constant pain • is too large to pass on its own or is caught in a difficult place • blocks the flow of urine • causes ongoing urinary tract infection • damages kidney tissue or causes constant bleeding • has grown larger (as seen on follow-up x ray studies).
Surgical options Surgical options include: -Extracorporeal shockwave lithotripsy (ESWL): It is the most frequently used procedure for the treatment of kidney stones. In ESWL, shock waves that are created outside the body travel through the skin and body tissues until they hit the denser stones. The stones break down into sand-like particles and are easily passed through the urinary tract in the urine. -Percutaneous nephrolithotomy: It is recommended to remove a stone that is quite large or in a location that does not allow effective use of ESWL. -Ureteroscopic Stone Removal: If a stone is located low in the urether, it might not be amenable to ESWL. A small fiberoptic instrument called a ureteroscope is passed through the urethra and bladder into the ureter and the stone is either mechanically extracted or fragmented with shock wave impulse
2. Which of the following factors is not associated with calcium stones • High uricosuria • High Na diet • High oxaluria • High citraturia • Alkaline pH Go to the next slide for the answer
Answer: d. Uric acid acts as a nidus for calcium stones. High Na diet leads to increased urinary calcium. Oxalate binds to calcium in the urine and precipitates calcium-oxalate crystals if present at high concentrations. Alkaline pH precipitates calcium stones. Citrate is the most powerful inhibitor of calcium oxalate stones
3. True or False. In patients with calcium oxalate stones, decreasing calcium intake will lower urinary calcium excretion and will result in less stone formation. Go to the next slide for the answer
Answer: False. Lowering calcium intake will result in less calcium chelating oxalate in the GI tract, more oxalate absorption and thus urinary excretion. Hyperoxaluria will cause more calcium stone precipitations
4. True/False: Potassium citrate is routinely used in patients with calcium oxalate stones and low urinary citrate. Go to the next slide for the answer
4. Answer: False. Although citrate is a powerful inhibitor of calcium oxalate formation and needed in the urine to prevent stones, it also raises the pH which might cause more calcium stone precipitation, especially calcium phosphate. If the urine pH >6, it should be avoided.
References: • Pictures of kidney stone crystal morphology are taken from the following site: www.Uptodate.com / Clinical evaluation of kidney stones • Straub M. Hautmann RE. Developments in stone prevention. Curr Opin Urol. 2005 Mar;15(2):119-26. • Knoll T, Zollner A. Cystinuria in childhood and adolescence: recommendations for diagnosis, treatment, and follow-up. Pediatr Nephrol. 2005 Jan;20(1):19-24. • Rao PN. Imaging for kidney stones. World J Urol. 2004 Nov;22(5):323-7. • Caramia G, Di Gregorio L, et. al. Uric acid, phosphate and oxalate stones: treatment and prophylaxis. Urol Int. 2004;72 Suppl 1:24-8. • Marangella M, Bagnis C, et. al. Crystallization inhibitors in the pathophysiology and treatment of nephrolithiasis. Urol Int. 2004;72 Suppl 1:6-10 • Amato M, Lusini ML. Epidemiology of nephrolithiasis today. Urol Int. 2004;72 Suppl 1:1-5. • Putmann SS, Hamilton BD. The use of shock wave lithotripsy for renal calculi. Curr Opin Urol. 2004 Mar;14(2):117-21 • Sandhu C, Anson KM. Urinary tract stones--Part I: role of radiological imaging in diagnosis and treatment planning. Clin Radiol. 2003 Jun;58(6):415-21. • Sandhu C, Anson KM Urinary tract stones--Part II: current status of treatment.Clin Radiol. 2003 Jun;58(6):422-33. Review.