Download
1 / 51
520 likes | 734 Vues
Role of proteolysis in physiological and pathological processes. Zdenka Kučerová. Proteolytic enzymes :. cleave peptide bonds ( proteins or peptides ) control of the cell cycle key roles in many pathophysiological processes targets for therapeutic strategies

E N D
Role of proteolysis in physiological and pathological processes Zdenka Kučerová
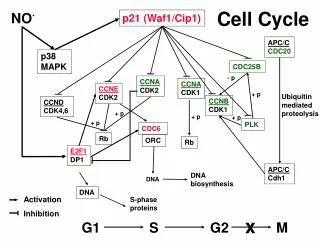
Proteolyticenzymes : • cleave peptide bonds ( proteinsorpeptides) • control of the cell cycle • key roles in many pathophysiological processes • targets for therapeutic strategies • speed of the cleavage depends on the strategically located positions of cleaved bonds
Activity of proteolytic enzymes • determined by many factors at the post-translational level • allosteric nature physiologically important interactions • explains why the enzymes carry a large body of structural and functional information • degradom
Regulation by proteolytic enzymes • limited proteolysis or by proteinase inhibitors • Limited proteolysis: • post-translational modification • conversion of an inactive precursor into an active form • Proteinase inhibitors: • regulate:coagulation • fibrinolysis • connective tissue turnover • complement activation • concentration changes during physiological or pathological processes
Proteolysis • complete degradation of proteins to free amino acids • requires series of enzymes with different specificity • not only in the digestive tract, but also in every cell in lysosomes, in cytoplasm and other parts of the cell • Division of proteolytic enzymes peptidasesendopeptidases and exopeptidases (position of the cleavage site within the substrate molecule) • endopeptidases(proteinases) groups according to similar reaction mechanisms (e.g. serine or cysteine proteinases)
Mechnism of interaction • enzymes recognise and bind to a short amino acid sequences and then specifically hydrolyse bonds between particular aminoacid residues
Classification of proteinases A) endopeptidases – hydrolysis within the peptide chain 1)serine proteinases – serine or histidine residues in active sites, pH optimum 7 – 9 trypsin, chymotrypsin, thrombin, plasmin 2)cysteine proteinases – cysteine residue in active site, pH optimum 4 – 7 calpain, caspases 3)aspartic proteinases – two aspartic residues in active site, pH optimum below 5 pepsin, gastricsin, rennin, HIV proteinase 4)metaloproteinases – metal ion important for catalysis, pH opt. 7 – 9 matrix metaloproteinases, collagenase, gelatinase
B)exopeptidases - cleave off single amino acid one after another • 1)aminopeptidases – cleave off a single amino acid from amino terminus • 2)dipeptidyldipeptidases – cleave off dipeptide from amino terminus • 3)carboxypeptidases – cleave off a single amino acid from carboxy terminus • 4)dipeptidases – hydrolyse dipeptides in two single amino acids • Individual proteinases differ in their substrate specifity • For complete degradation of a protein, enzymes from each of the above-named groups are required
Characterization of some proteinases enzym m.wt isoelektric point (pH) chymotrypsino- gen 25.000 8.1 trypsin 24.000 10.8 plasmin 75.000 - elastase 26.000 9.5 papain 21.000 8.7 pepsin 33.000 1.0 carboxypepti- 34.000 6.0 dase A
Inhibitors • differ according to individual groups of proteinases • Serine proteinases…..chlormethylketons, • Cysteine proteinases…. dithiothreitol, mercaptans, • Aspartic proteinasess… epoxy- and diazo- compounds, pepstatin • Metalloproteinases….. chelates
Serine proteinases • Proteinases of digestive tract – trypsin, chymotrypsin • important for: • fibrinolysis • blood coagulation • complement activation • produced as inactive zymogens • activated by limited proteolysis by another proteinase
Blood clotting • enzymatic conversion of a soluble plasmatic fibrinogen into a fibrous network of insoluble fibrin polymers • fibrinogen cleaved by thrombin and fibrin aggregate into insoluble fibrin polymer • most of the coagulation factors are proteinases
Initiation of blood clotting • two different ways • extravascular pathway- triggered by an injury of tissue • intravascular pathway- initiated by contact with a damaged inner surface of blood vessel • cascade of proteolytic cleavages • requires calcium and phospholipids • conversion of inactive prothrombin to active thrombin • series of zymogens of serine proteinases are sequentially activated (active serine proteinases arise from inactive precursors, the active enzymes then activate other inactive proteins)
Unique aspects of coagulation • requirement for a protein or a lipoprotein cofactor for optimal reaction rates • requirement for a membrane surface • metal ion requirement • uniqueness of initiating reactions in comparison to those which activate the pancreatic zymogens
Blood coagulation cascade • ended by dissociation of the membrane complex • regulated by activators and inhibitors in dynamic equilibrium • Antithrombin III • inhibits activity of thrombin an anticoagulant factor • anticoagulant therapy reduction of formation or reduction of function of thrombin and other serine proteinases • Protein C • Serine proteinase…inactivation of factor Va and VIIIa
Fibrinolysis • fibrin networks are degraded by plasmin • plasmin is serine proteinase • plasmin evolves from precursor plasminogenafter activation by plasminogen activator • plasmin activity inhibited by α-2 antiplasmin • therapy by fibrinolytic proteinases thrombus degradation
Characterization of plasmin, plasminogen and plasminogen activator Plasminogen is one-chain glykoprotein hydrolyse bounds Arg67-Met68, Lys76-Lys77, Lys77-Val78 Plasmin is two chain serine protease (with disulfidic bound) active site His-603, Asp-646, Ser-741 its main target is fibrin Human plasminogen activator [PA] is serine protease (tissue and urokinase) one polypeptide chain ( single chain-ScuPA) hydrolyse bounds Arg275-Ileu276(two chain-TctPA)
plasmin formation is dependent on: • plasmatic concentration of plasminogen • availability of activators of plasminogen in the plasma • surrounding tissue environment • concentration of naturally present inhibitors • concentration of fibrin
Pathological fibrinolysis • abnormal fibrinolysis, bleeding or thrombus formation • Higher fibrinolysis • increased level of plasminogen activator (PA) • deficiency of plasminogen activator inhibitor (PAI) • deficiency of antiplasmin • Thrombus formation • defective synthesis of plasmin or PA • PA used to pharmacological digestion of thrombus • Malignant tumors • disorders of hemostasis - ability of the tumor to alter the coagulation system
Tumor malignanciesconnected with invasive growth and metastasisenzymatic breakdown of two proteolytic systems (fibrinolytic s. and matrix metaloproteinases s.) • Methastatic disease • disintegrated regulation • irreversible progression of cell cycle • resistance to a cell signalling • understanding of the mechanismpreventing tumor cell spread • proteases have proteolytic activity that may affect cancer progression
Proteinases - Biomarkers • correspond to changes in the whole organism • changes: - biochemical • - histological • - morphological • - physiological • very important for early diagnosis
Complement • This system collaborates in recognition and elimination of pathogens as a part of both the innate and acquired immune systems. • The activation of complement pathway - through attached serine proteases • the complement system is one of the most highly organized innate immune systems • serine proteinases are responsible for regulation of the early event of complement
Kallikrein • plasmatic serine proteinases (15 ) • kalikrein - kinin is a complex system produced in various organs • the kallikreins must now be considered as important 'hormonal' regulators of tissue function • important for initiation of cellular fibrinolysis, which is independent on plasmin, fibrin and tissue plasminogen activator • predictive marker for cancer
Cysteine proteinases • lysosomal- cysteine cathepsins • implicated in tumor spread and metastasis • prognostic factors for tumor recurrence in human breast cancer • non-lysosomal – calpain • cleave cell-cycle proteins, cytoskeletal and myofibrilar proteins • cytoplasmatic enzyme
Apoptosis • evolutionary conserved form of cell suicide • requires a proteolytic system - mainly caspases • caspase family of proteases can be divided into pro-apoptotic and pro-inflammatory members based on their substrate specificity and participation in separate signalling cascades • caspase regulation therapeutic purposes • caspases -minimally requires a tetrapeptide substrate in which Asp is in absolute requirement in P1 position, the P4 substrate residues is unique to each homologue.
defective control of apoptosis pathogenesis of diseases • cancer chemotherapy and radiation cancer cell death by apoptosis • Caspases are responsible for crucial aspects of inflammation and immune-cell death that are disrupted in a number of genetic autoimmune and autoinflammatory diseases. • caspases proteolytic devitalizing and remodelling of tumor cellssuppress tumor cell growth invasion and metastasis
Aspartic proteinases • Acid proteinases from mammalian gastric mucosa pepsins • Proteinases associated with limited proteolysis renin blood pressure cathepsins D,E lysosomal enzyme proteinase HIV
Renin • aspartic proteinase • formed as a precursor (prorenin) in kidneys • active form (renin) released into the blood • renin cleaves angiotensinogen to form angiotensin I • angiotensin-converting enzyme (ACE) then converts angiotensin I to angiotensin II
Renin • highly specific • synthesized in response to decreasing levels of sodium ions and declining blood pressure • renin angiotensin II affects:- kidney • - brain stem • - hypophysis • - adrenal cortex • - blood vessel walls • - heart
Cathepsins D and E • Cathepsin D • aspartic proteinase localized in lysosomes • in most tissues and cells of human organism • widely distributed among biological species • influences:- intracellular protein catabolism • - hormone and antigen processing • - pathological processes (neoplasia and • neurodegenerative changes) • Cathepsin E • in human stomach cells (another stomach cells than pepsinogen and progastricsin) • Both is over- expressed by cancer cells
Proteinase HIV • AIDS retrovirus (human immunodeficiency virus) • retroviral aspartic proteinases deeply studied proteins in today molecular biology chemistry • three-dimensional structure of active site is similar to that of eucariotic proteinases • proteinase (and other enzymes)design of novel drugs for the treatment of AIDS • fast development of resistance of virus towards synthetic inhibitors and low bioavailability of these inhibitors • resistance results primarily from multiple mutations of the proteinase
drug-resistant HIV proteinase →altered substrate specifity • altered substrate specifity understanding→valuable in the design of new protease inhibitors • active antiretroviral therapy (HAART) combining potent drugs that can inhibit reverse transcriptase, integrase and protease activities
Metaloproteinases • matrix metaloproteinases (MMPs) • zinc-dependent enzymes • regulate tissue remodelling in physiological and pathological conditions • MMPs are key enzymes for tumor progression cell carcinoma • individual MMPs found in most tumor types • presence of specific MMPs has been shown to be a prognostic marker at tumor invasion • tumor invasion and metastasis→ degradation of the extracellular matrix around tumor cells and cell migration
cancer metastasis →imbalance between MMPs and its inhibitor • MMPs→ regulatory effects on both primary and secondary tumors • inhibitors of MMPs were assessed for anticancer properties • proteolysis has a central role for cancer metastasis
Exopeptidases • Peptidyl dipeptidases • angiotensin-converting enzyme in the control of blood pressure • Human prolylcarboxypeptidasealso known as angiotensinase C inactivates angiotensin II • Inhibitors of dipeptidyl peptidase IV (DPP IV) provide a strategy for the treatment of type 2 diabetes • Methionine aminopeptidase (MetAP) is a bifunctional protein that plays a critical role in the regulation of post-translational processing and protein synthesis • inhibitors of all peptidases have therapeutic effect
Human gastric proteinases • digestive proteinases • adult mammalian gastric mucosa contains the highest concentration and greatest diversity of gastric proteinases • human gastric mucosa contains four aspartic proteinases: - pepsinogen A (PGA) • - pepsinogen C (PGC) • -chymosin • - cathepsin E • common biological properties (the ability to hydrolyze proteins at acid pH) but each is distinguishable by immunologic technique • serum contains both PGA and PGC, but only PGA is detectable in urine
Pepsinogen A and pepsinogen C • aspartic proteinases • differ in charge → distinguishable by electrophoresis • heterogeneity of pepsinogens → multiple genes • →posttranslational modifications of the primary gene product
Duodenal ulcer • high level of PGA → subclinical marker of duodenal ulcer • Superficial gastritis • acute or chronic superficial gastritis → high serum PGA and PGC levels • inflammation of the mucosa→ increased rates of release of both zymogens into the circulation → elevated levels of PGA and PGC • level of PGC increased much more than level of PGA
Pepsinogen A / pepsinogen C ratio in peptic ulcer, gastric cancer and control
Gastric ulcer • changed levels of PGA and PGC • gastric ulcer usually develops within areas of chronic gastritis • pepsinogen A / pepsinogen C ration decreases
Gastric cancer • very low serum levels of PGA • low serum PGA level → subclinical marker of increased risk for gastric cancer→ it is possible to identify high-risk subjects→ more effective approaches to diagnosis and treatment • serum PGA and PGC levels → subclinical markers of disorders of gastric mucosal structure and function