Download
1 / 31
310 likes | 513 Vues
Mutations at the level of the homologous pair. EUPLOIDY : "true" ploidy , meaning two members of each homologous pair. ANEUPLOIDY : "not true" ploidy , meaning more or fewer members than two of each homologous pair. MONOSOMY - one homolog; partner is missing TRISOMY - three homologs

E N D
Mutations at the level of the homologous pair EUPLOIDY: "true" ploidy, meaning two members of each homologous pair. ANEUPLOIDY: "not true" ploidy, meaning more or fewer members than two of each homologous pair. MONOSOMY - one homolog; partner is missing TRISOMY - three homologs NULLISOMY- one entire homologous pair is missing.
Trisomy: Patau Syndrome • 1/20,000 births • severe mental retardation • heart and organ defects • polydactyly • death by the age of one year
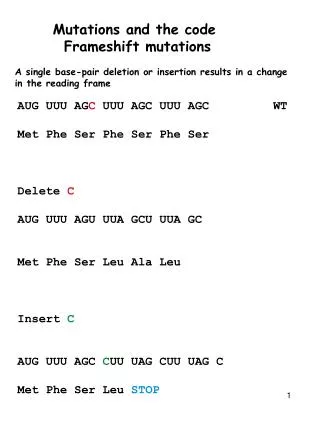
How can chromosomes break? Ionizing radiation (production of free radicals, which act like little atomic "cannon balls", blasting through strands of DNA or c'somes. Chemical insult.
Why do they rejoin? • Break points of chromosomes are highly reactive ("sticky"), whereas normal ends of c'somes are capped by telomeres, which do not readily bond to other molecules.
Structural Changes • Deletions (deficiencies) • Duplications • Inversions • Translocations
Cri-du-chat Syndrome Mental retardation Slow motor skill development Low birth weight and slow growth Small head (microcephaly) Partial webbing of fingers or toes Wide-set eyes (hypertelorism) High-pitched cry
Possible neonatal features: • Lymphoedema, webbed neck, coarctation of the aorta, renal anomalies Other features include: • Short stature, infertility due to streak gonads or premature ovarian failure (if mosaic TS), educational or behavioural problems
45,X Turner syndrome (a) Puffy feet. (b) redundant skin at back of neck. (c) Histology of gonads: ovarian cortical strome devoid of germ cell elements
Down Syndrome • 1 in 700 live births • >60% spontaneously aborted • 20% stillborn • Facial appearance permits diagnosis • Marked muscle hypotonia as baby • Single palmar crease may be present • Learning difficulty (IQ usually <50) • Congenital heart malformations (40%) • Many other associated features
Trisomies appear to be associated with an increase in maternal age • The trisomy 21 type of Down syndrome is the result of an error in meiosis, and has a recurrence risk of about 1 in 100.
Interphase FISH test for trisomy 21 • The chromosome 21 probe is labelled with a red fluorochrome and a control probe (for chromosome 18) is labelled in green. The two green dots show that the hybridization has worked for this cell, and the three red dots show that there are three copies of chromosome 21. The clinical report is based on examining a large number of cells. For prenatal diagnosis a mix of differently coloured probes from chromosomes 13, 18, 21, X and Y is often used.
Clinical Features • Head and neck • Brachycephaly • Up-slanting palpebral fissures • Epicanthal folds • Brushfield spots • Flat nasal bridge • Folded or dysplastic ears • Open mouth • Protruding tongue • Short neck • Excessive skin at the nape of neck
Extremities • Shortbroad hands • Short fifth finger • Incurved fifth finger • Transverse palmer crease • Space between first and second toe • Hyper flexibility of joints
Mental Retardation • Almost all DS babies have MR. • Mildly to moderately retarded . • Starts in the first year of life. • Average age of sitting(11 mon), and walking (26 mon) is twice the typical age. • First words at 18 months. • IQ declines through the first 10 years of age, reaching a plateau in adolescence that continues into adulthood.
Heart Disease • 50 % of Down Syndrome pts have heart disease • Atrioventricularseptal defect • VSD • Secundum ASD • PDA • Tetrology of Fallot • Mitral valve prolapse • AR, MR
GI abnormalities • 5% of cases • Duodenal atresia or stenosis, sometimes assoc with annular pancreas in 2.5 % of cases • Imperforate anus • Esophageal atresia with TE fistula is less common • Hirschsprung’s disease • Strong assoc with celiac disease b/w 5 – 16 % , 5 – 16 fold increase as compared to general population
Growth • BW, length and HC are less in DS • Reduced growth rate • Prevalence of obesity is greater in DS • Weight is less than expected for length in infants with DS, and then increases disproportion ally so that they are obese by age 3-4 yrs
Alzheimer’s disease – Adult with a Down Syndrome has earlier onset of symptoms. When diagnosis is considered, thyroid disease and possible depression should be excluded.
Klinefelter Syndrome Clinical Features • Hypogonadism • Reduced testosterone levels • Infertility • Tall stature • Gynaecomastia • Educational difficulties – Intelligence can be 10-15 points lower than siblings but usually in normal range • Behavioural problems.