Aprotinin Observational Studies
300 likes | 446 Vues
The September 12, 2007, meeting led by Rita Ouellet-Hellstrom, Ph.D., M.P.H. from FDA/CDER focused on safety concerns regarding Aprotinin, identified through observational studies. Key issues included cardiovascular, cerebrovascular, renal events, and in-hospital deaths linked to Aprotinin use. Discussions covered study design, bias, adjustment tools, and the consistency of published results. A re-analysis or clinical trials were proposed as next steps to validate findings. The complexities of observational studies emphasize the need for rigorous testing and comprehensive follow-up to better understand Aprotinin's risk profile.

Aprotinin Observational Studies
E N D
Presentation Transcript
Aprotinin Observational Studies Advisory Committee Meeting - September 12, 2007 Rita Ouellet-Hellstrom, Ph.D., M.P.H. FDA CDER Office of Surveillance and Epidemiology Division of Drug Risk Evaluation (DDRE)
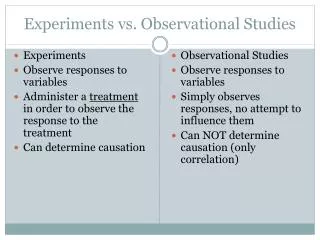
Objectives • Safety concerns identified by observational studies (cardiovascular, cerebrovascular, renal events and in-hospital deaths) • Design, exposure & outcome definitions, potential bias, adjustment tools • Consistency of the published results • Next step - Re-analysis or clinical trials
Issues - Observational Studies • Study Design • Types of procedures performed • Population size • Control or comparator group(s) • Exposure & outcome definitions
Selected Hemostatic Agents; Premier Network of Hospitals, 2000 – 2006 by QuarterCardiovascular System
Percent Lost-to-Follow-upby Treatment Group Mangano et al. JAMA; 297(5):471-479, Feb 2007
Confounders & Bias • Utilization codes • Imbalance of baseline characteristics across treatment groups • Channeling bias • Geographical, institutional, and provider clustering • Time-to-event analyses • Comprehensive follow-up
Utilization CodesIdentify Outcomes & Confounders • Myocardial Infarction • Sensitivity - 67% • Specificity - 100% • Thrombolysis in ischemic stroke • Sensitivity - 55% • Specificity - 98% • Non-specific codes for heart failure, renal dysfunction McAlpine R et al. Pharmacoepidemiol & Drug Safety, 7:311-318, 1998 Qureshi AI et al. J Clin Epidemiology, 59:856-858, 2006
Adjustment Tools • Multivariate Modeling • Logistic regression (all) • Proportional hazard regression (time) • Conditional logistic regression (matching) • Matching/Stratifying • Propensity Scores • Design • Analysis
Observation Time - Hospital Stay • Short-term • Longer hospital stays • Increase the probability of having an outcome observed • Early discharge to other facilities • Missing observations • Average length of stay specified by Karkouti • 8 days for each treatment group & a range of 6-13 days for aprotinin & 6-12 days for tranexamic acid • Long-term • Lost-to-follow-up • Competing co-morbidities
Re-analysis Can: • Reproduce study results • Standardize analytical approaches • Assess comparability of risk across treatment groups • Perform time-to-event analyses • Compare aprotinin treatment with no treatment
Re-analysis Cannot: • Re-define outcome & exposure criteria • Provide missing information • On patients from excluded centers • Patients lost-to-follow-up • Uncollected data identifying co-morbidity & competing risks in long-term follow-up
Summary - Observational Studies • Different designs & outcome definitions • Some studies with large number of patients • Others with access to medical records & some with direct patient contact • Consistency of results for renal events • Suggestive but inconclusive results on in-hospital deaths, cardiovascular & cerebrovascular events • Re-analysis provides some answers but final results may have to await a large study powered to assess safety & death