Download
1 / 28
280 likes | 309 Vues
Explore the mechanisms and clinical applications of Vitamin K antagonist Warfarin and Factor Xa Inhibitor Rivaroxaban in managing clotting disorders. Learn about pharmacokinetics, indications, adverse effects, and more.

E N D
Clinical Use of Coagulation Inhibitors Aleksandra Milosevski Shi Yi Chen Ya Ping Guo Vanessa Hoi PHM142 Fall 2019 Instructor: Chesa Dojo Soeandy • Coordinator: Jeffrey Henderson
Coagulation Cascade Overview - Silverthorn, Fig. 16.4
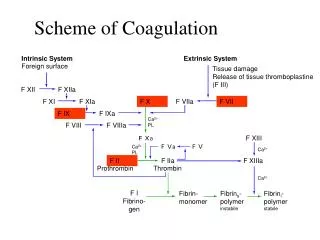
Extrinsic Pathway • Tissue Factor (III) → found in tissue underlying blood vessels • Tissue Factor (III) + Active VII Form Complex • End result → X activated • Positive feedback observed Silverthorn, Fig. 16.4
Intrinsic Pathway • Blood vessel damage exposes collagen • Factors XII, XI, IX, VII activated • Factor X also activated Silverthorn, Fig. 16.4
Common Pathway Silverthorn, Fig. 16.4 • Active Factor X cleaves prothrombin → thrombin • Fibrinogen → Fibrin • Factor XIII also activated
Vitamin K in Coagulation Cascade • Protein carboxylation reaction activates the clotting factors • Coupled to the oxidation of vitamin K • Vitamin K is reused • Must be reduced to reactivate it via VKOR • Warfarin: Vitamin K antagonist Silverthorn, Fig. 16.4
Vitamin K in Coagulation Cascade • Protein carboxylation reaction activates the clotting factors • Coupled to the oxidation of vitamin K • Vitamin K is reused • Must be reduced to reactivate it via VKOR • Warfarin: Vitamin K antagonist • Inhibit VKOR • Inhibition of VKOR → inhibits reactivation of vitamin K → decreases the synthesis of clotting factors VKOR Katzung, Fig. 34.6
Warfarin: Vitamin K antagonist • Clinical Use: • Prophylaxis and/or treatment of venous thrombosis • Atrial fibrillation • Prosthetic heart valves • Pharmacokinetics: • Completely absorbed after oral administration • Biotransformed in liver and excreted by the kidney • Very little Warfarin is excreted unchanged in the urine → elimination by metabolism • 8-12h delay in the action of warfarin • Peak anticoagulant effect may be delayed 3-4 days • Half-life: 20-60h • Over 99% of the drug is bound to plasma albumin
Adverse Effects & Warnings/Precautions • Excessive bleeding • Reversed by stopping the drug and administering vitamin K, fresh-frozen plasma • Narrow therapeutic index • Requires frequent monitoring • Dosing is affected by polymorphism of the CYP2C9 enzyme and VKOR • Dose is individualized • Can cross placenta • Cause birth malformations and fatal hemorrhage in fetus • Up to 160 drugs would have potential drug interaction with warfarin such as acetaminophen and amoxicillin (CYP2C9, VKOR) • 46 reported to have interactions such as atorvastatin and ranitidine
Direct Factor Xa Inhibitors (Rivaroxaban, Apixaban, Edoxaban) • Activation of Factor-X to Factor-Xa (FXa) • FXa and FVa form prothrombinase complex • Converts prothrombin to thrombin • Ultimately increases clot formation Silverthorn, Fig. 16.4 Perzborn, Fig. 1 • Coagulation cascade exhibits amplification • FXa causes an explosive burst of thrombin and clot formation Wheeless, 2015
Direct Factor Xa Inhibitors (Rivaroxaban,Apixaban, Edoxaban) • Activation of Factor-X to Factor-Xa (FXa) • FXa and FVa form prothrombinase complex • Converts prothrombin to thrombin • Ultimately increases clot formation Silverthorn, Fig. 16.4 Perzborn, Fig. 1 • Coagulation cascade exhibits amplification • FXa causes an explosive burst of thrombin and clot formation Inhibition of FXa terminates thrombin generation and decreases coagulation. Wheeless, 2015
Rivaroxaban is a highly selective, competitive, direct, antithrombin-independent Factor Xa inhibitor. Binds free FXa and FXa bound in Prothombinase. Perzborn, Fig. 2
Indications and Clinical Use • Rivaroxaban 10 mg, 15 mg, and 20 mg is indicated for: • prevention of venous thromboembolic events (VTE) in patients after total hip or knee replacement surgery • treatment of VTE like deep vein thrombosis (DVT) and pulmonary embolism (PE), and prevention of recurrence • prevention of stroke and systemic embolism in patients with non-valvular atrial fibrillation (AF) • No data to support safety and efficacy in patients with prosthetic heart valves • Rivaroxaban 2.5 mg in combination with 75 mg-100 mg acetylsalicylic acid is indicated for: • prevention of stroke, myocardial infarction, and cardiovascular death • prevention of acute limb ischemia and mortality in coronary artery disease (CAD)
Pharmacokinetics of Rivaroxaban Elimination • Approximately 1/3 of dose eliminated as unchanged active drug by kidneys • 30% via active renal secretion, transporters involved are P-glycoprotein (P-gp) and breast cancer resistance protein (BCRP) • 6% via glomerular filtration • Approximately 2/3 of dose metabolically deactivated • CYP 3A4/5 and CYP2J2 viahepatic oxidative biotransformation • CYP-independent hydrolysis of amide bonds • Resulting metabolites eliminated renally and via the hepatobiliary route • Half-life: 5–9 hours (shorter than warfarin) Absorption, Bioavailability, Protein Binding, Distribution • High Oral Bioavailability (Foral): • 2.5 mg, 5 mg, 10 mg (with or without food) or 20 mg (with food): 80% - 100% • 20 mg (without food): 66% • Peak plasma level (tmax): 2 – 4 hours • High reversible plasma protein binding • approximately 92–95 %in vitro • mainly bound to serum albumin • Volume of distribution at steady state = 50 L (0.62 L/kg) • low-to-moderate affinity to peripheral tissues
Pros & Cons CONS • no standardized test should monitoring be needed • expensive PROS • wide therapeutic window and predictable pharmacokinetics • fixed-dose oral administration regimens that do not require monitoring • limited known drug interactions and no known dietary restrictions • Andexanet, a FXa decoy, recently approved as antidote
Adverse Reactions/Contraindications/Warnings Adverse Reactions • increased risk of bleeding which can result in weakness, paleness, dizziness, or swelling and secondary complications like renal failure Contraindications • no data to support use in children; pregnant or nursing women; patients with prosthetic heart valves; patients with clinically significant bleeding (ulcers, cerebral infarction etc.) Warnings and Precautions • concomitant use with strong inhibitors of CYP3A4 and P-glycoprotein (ketoconazole, itraconazole, posaconazole, ritonavir) • concomitant use with any other hemostasis-affecting drugs (non-steroidal anti-inflammatory drugs, acetylsalicylic acid, platelet aggregation inhibitors or selective serotonin reuptake inhibitors, and serotonin norepinephrine reuptake inhibitors) • hepatic disease and renal impairment; must first determine creatinine clearance in all patients
Heparin • Mixture of mucopolysaccharides • Co-factor of anti-thrombin • Target: Thrombin Silverthorn, Fig. 16.4
Heparin: Mechanism of Action • Enhance Anti-Thrombin Activity by 1000 times • Inhibit thrombin • Inhibit factor X Anti-Thrombin Slow Silverthorn, Fig. 16.4
Heparin: Mechanism of Action • Enhance Anti-Thrombin Activity by 1000 times • Inhibit thrombin • Inhibit factor X Heparin Anti-Thrombin Silverthorn, Fig. 16.4
Heparin: Mechanism of Action • Enhance Anti-Thrombin by 1000 times • Inhibit thrombin • Inhibit factor X Heparin Anti-Thrombin Silverthorn, Fig. 16.4
Heparin: Clinical Use • Administration and onset • IV: immediate • Deep subcutaneous: might be delayed 20-60 mins • No oral: Negatively charged and large • Half-life: 90 mins • Commonly used for • Cardiac surgery • Prevention of venous thromboembolism
Heparin: LMWH • Low molecular weight heparin (LMWH) • Fragmented heparin • Weaker anticoagulation • CANNOT inactivate thrombin • CAN inactivate Factor X c c Heparin Anti-Thrombin Silverthorn, Fig. 16.4
Heparin: LMWH • Low molecular weight heparin (LMWH) • Fragmented heparin • Weaker anticoagulation • CANNOT inactivate thrombin • CAN inactivate Factor X c only Heparin Anti-Thrombin Silverthorn, Fig. 16.4
Heparin: LMWH vs. unfractionated • More predictable pharmacokinetic • No monitoring is required • Different onset and half-life: not interchangeable
Summary Warfarin Direct Factor Xa Inhibitor (Rivaroxaban) Heparin
References CPS [Internet]. Ottawa (ON): Canadian Pharmacists Association; c2016 [updated 2018 SEP 04; cited 2019 SEP 16]. Coumadin [product monograph]. Available from: http://www.e-cps.ca or http://www.myrxtx.ca. CPS [internet]. Ottawa (ON): Canadian Pharmacists Association; c2016 [updated 2016 DEC; cited 2019 SEP 16]. Heparin: unfractionated. Available from: http://www.e-cps.ca or http://www.myrxtx.ca. CPS [internet]. Ottawa (ON): Canadian Pharmacists Association; c2016 [updated 2015 JUN; cited 2019 SEP 16]. Heparin: low molecular weight. Available from: http://www.e-cps.ca or http://www.myrxtx.ca. CPS [Internet]. Ottawa (ON): Canadian Pharmacists Association; c2016 [updated 2018 SEP 18; cited 2019 SEP 16]. Xarelto [product monograph]. Available from: http://www.e-cps.ca or http://www.myrxtx.ca. Katzung, B.G. (2018). Basic and Clinical Pharmacology, 14th Edition. McGraw Hill Education. Perzborn Elisabeth, Roehrig Susanne, Straub Alexander, Kubitza Dagmar, Mueck Wolfgang, and Laux Volker. “Rivaroxaban: A New Oral Factor Xa Inhibitor” Arteriosclerosis, Thrombosis, and Vascular Biology. 30.3 (2010): 376–381. Web. 16 Sep. 2019. Silverthorn, D.U. (2012). Human Physiology: An Integrated Approach, 8th Edition. Pearson Education.