Download
1 / 1
10 likes | 175 Vues
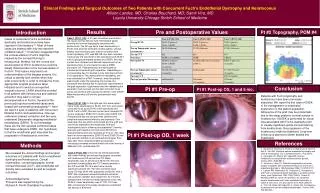
Clinical Findings and Surgical Outcomes of Two Patients with Concurrent Fuch’s Endothelial Dystrophy and Keratoconus Allison Landes, MD; Charles Bouchard, MD; Samir Vira, MD Loyola University Chicago Stritch School of Medicine. Results. Pre and Postoperative Values. Pt #2 Topography, POM #4.

E N D
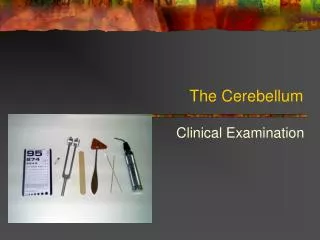
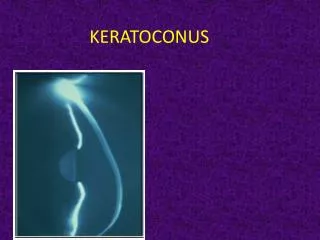
Clinical Findings and Surgical Outcomes of Two Patients with Concurrent Fuch’s Endothelial Dystrophy and Keratoconus Allison Landes, MD; Charles Bouchard, MD; Samir Vira, MD Loyola University Chicago Stritch School of Medicine Results Pre and Postoperative Values Pt #2 Topography, POM #4 Introduction Case 1 (Pt #1, OS): A 41 year old woman presented to the Loyola Cornea Service with mild bilateral apical scarring and corneal topography consistent with keratoconus. The left eye had a mean keratometry of 56.0D. She also had confluent corneal guttata, stromal edema, and mild microcystic edema consistent with Fuch’s dystrophy. CCT was 662 OS. Her best corrected visual acuity OS was 20/40-2 with spectacles and 20/30-1 with a rigid gas permeable contact lens (RGP). She was contact lens intolerant and desired improvement in her spectacle vision, so she elected to have a DSEK procedure OS. Postoperatively, she developed an inferotemporal sectoral graft separation. Rebubbling on post-operative day 16 resulted in only mild improvement in the separation. Two weeks after the rebubbling, she was scheduled for a PKP. However, when the patient was brought under the operating microscope, the procedure was aborted due to significant improvement of the graft separation. Eight weeks after the rebubbling the separation had resolved and her best corrected visual acuity was 20/40+2 with glasses and 20/30-1 with a RGP. Mean keratometry at 6 months postoperative was 50.21D. Cases of concurrent Fuch’s endothelial dystrophy and keratoconus have been reported in the literature1-6. Most of these cases are bilateral with only two reported unilateral cases1,2. It has been suggested that the corneal edema in Fuch’s might be masked by the corneal thinning in keratoconus; likewise, the thin cornea one would expect to find in keratoconus could be falsely thickened due to the corneal edema of Fuch’s3. This feature may lead to an underestimation of the disease severity. It is critical to identify both entities when they exist concurrently in order to choose the most appropriate surgical procedure when indicated and to avoid an unexpected surgical outcome. LASIK should be avoided in all patients with keratoconus and cataract extraction may lead to corneal decompensation in Fuch’s. Several of the previously reported combined cases were treated with penetrating keratoplasty4,5. Here we report 4 eyes (2 patients) with concurrent bilateral Fuch’s and keratoconus. One eye underwent cataract extraction and two eyes underwent Descemet’s stripping endothelial keratoplasty (DSEK). To our knowledge, these are the first reported combined cases that have undergone DSEK. Our hypothesis is that the endothelial graft may slow the progression of keratoconus over time. Conclusion Pt #1 Pre-op Pt #1 Post-op OS, 1 and 6 mo. Patients with Fuch’s dystrophy and keratoconus have been previously described. We report the first case of DSEK in the management of endothelial dysfunction in this patient population. Adherence of the graft may be problematic due to the steep posterior corneal surface in keratoconus. If DSEK is performed for visual loss associated with Fuch’s dystrophy prior to visually significant apical corneal scarring from keratoconus, the progression of the keratoconus might be stabilized. Long term follow up is planned to better assess this hypothesis. Case 2 (Pt #1 OD): In the right eye, this same patient had a mean keratometry of 52.5D, CCT 610, and a best corrected visual acuity 20/40-2 with spectacles and 20/25-1 with a RGP. She was contact lens intolerant OD, so she underwent DSEK OD 5 months after DSEK OS. Postoperative day one the graft was centered with peripheral detachments inferiorly and superiorly. One week later she was 20/40 uncorrected and the graft was only mildly separated inferotemporally. She was subsequently lost to follow-up and presented 2 months later with graft rejection OU and vision 20/100 OU. Topical prednisolone was restarted q1-2 hours. Two days later her vision improved to 20/50 OD and 20/60 OS and she was also started on an oral prednisone taper. Four days later vision remained stable and specular microscopy revealed and endothelial cell count density of 2646/mm2 OD, unobtainable OS. Pt #1 Post-op OD, 1 week References Methods 1. Martone G, Tommasi C, Traversi C, Balestrazzi A, Berni E, Nuti E, Tosi GM. Unilateral corneal endothelial dystrophy and anterior keratoconus. Eur J Ophthalmol 2007; 17(3):430-2. 2. Darlington JK, Mannis MJ, Segal WA. Anterior keratoconus associated with unilateral cornea guttata. Cornea 2001; 20(8):881-4. 3. Jurkunas U, Azar DT. Potential complications of ocular surgery in patients with coexistent keratoconus and Fuch’s endothelial dystrophy. Ophthalmology 2006; 113:2187-2197. 4. Lipman RM, Rubenstein JB, Torczynski E. Keratoconus and Fuch’s corneal endothelial dystrophy in a patient and her family. Arch Ophthalmol 1990; 108(7):993-5. Salouti R, Nowroozzadeh M, Zamani M, ghoreyshi M. Combined anterior keratoconus and Fuch’s endothelial dystrophy: a report of two cases. Clin Exp Optom 2010; 93(4):268-270. 6. Orlin SE, Raber IM, Eagle RC Jr, Scheie HG. Keratoconus associated with corneal endothelial dystrophy. Cornea 1990; 9(4):229-304. We reviewed the clinical findings and surgical outcomes of 2 patients with Fuch’s endothelial dystrophy and keratoconus. Clinical examination, corneal topography, central corneal thickness (CCT), and endothelial cell density were evaluated as well as surgical outcomes. Acknowledgements: This work was supported by the Richard A. Perritt Charitable Foundation. Case 3 (Pt #2, OD): A 54 year old female presented with exam findings and corneal topography consistent with keratoconus OD worse than OS. Mean keratometry was 47.4D OD and 45.5D OS. She had confluent corneal guttata and CCT measurements of 614 OD and 595 OS. She also had a visually significant cataract OD. Her best corrected visual acuity OD was 20/40 with spectacles and 20/30- with a RGP. She underwent uneventful cataract extraction with posterior chamber lens implant OD. At 4 months postoperative, her best corrected spectacle vision was 20/25-2, mean keratometry was 47.17D, CCT was 609, and specular microscopy revealed an endothelial cell density of 929/mm2.