Download
1 / 16
170 likes | 654 Vues
Calcium channel blockers PHM 142. Matt Richler Stu Alp Pak Chan Jason Lee. PHM142 Fall 2012 Instructor: Dr. Jeffrey Henderson. Calcium channels.

E N D
Calcium channel blockersPHM 142 Matt Richler Stu Alp Pak Chan Jason Lee PHM142 Fall 2012 Instructor: Dr. Jeffrey Henderson
Calcium channels • Voltage-activated calcium channels regulate many intracellular processes, including contraction, secretion, neurotransmission, and gene expression • Composed of 4-5 subunits • α1 subunit incorporates the conduction pore • Site of pharmacological activity • Types of voltage-activated calcium channels: • L-Type: cardiac, skeletal, smooth muscle, neurons, endocrine cells, bone • T-Type • N-Type • P/Q-Type • R-Type
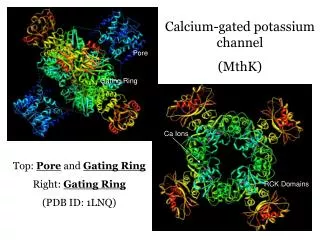
Calcium channels Subunit structure of CaV1 channels (L-type channels)
L-type Calcium channels • L-type physiology • The “L” in L-type stands for long acting in terms of the length of activation. • Like the other types of Calcium channels it is the α1 subunit that determines most of the channels properties • There are 4 sub types of L-Type calcium channels • CaV1.1 α1 Skeletal Muscle channel • CaV1.2 α1 Cardiac or Smooth Muscle channel • CaV1.3 α1 Neuroendocrine channel • CaV1.4 α1Retinal channel
L-Type subunits • CaV1.1 α1 • CaV1.1 α1 are only found in the transverse tubules of skeletal muscle and not in any other types of tissues • It initiates calcium release from the sarcoplasmic reticulum • CaV1.2 α1 Cardiac or Smooth Muscle channel • CaV1.2 α1 are found in large numbers in the cardiovascular system, smooth muscle, endocrine and neuroendocrine cells and in neurons • Most of the pharmacological effects of calcium channel blockers are believed to be almost exclusively mediated by CaV1.2 channels • CaV1.3 α1 Neuroendocrine channels • Cav1.3 is activated at more negative voltages than CaV1.2 channels and is activated more slowly • It is important in the control of resting heart rate. • CaV1.4 α1 • Important in Neurotransmitter release from photoreceptors
The Involvement of Voltage-Gated Calcium Channels in Cardiac Muscle Contraction
Maintenance of action potential by calcium channels • Prolong action potential in Cardiac Muscle • Act as a Target to drugs which block the Inward Ca+2 currents produced by Voltage-Gated Calcium Channels
Drugs • Dihydropyridines • Amlodipine • Nifedipine • Greater ratio of vascular smooth muscle effects relative to cardiac effects. e,g, vasodilators • Differ in their potency in different vascular beds • *dihydropyridines are CYP3A4 substrates; many potential interactions (e.g. Grapefruit juice)
Drugs • Non-Dihydropyridines • Verapamil • Diltiazem • More commonly used for cardiac effects – angina & cardiac dysrhythmias • Reduce cardiac contraction in a dose-dependent fashion • HR and cardiac output
Clinical Uses • Antihypertensives • Cardiac Dysrhythmias • Angina Pectoris
Antihypertensives • Inhibition of calcium influx into arterial smooth muscle cells • in [Ca2+]i results in smooth muscle long-lasting relaxation • Dihydropyridines, verapamil,diltiazem, are equally effective • Dihydropyridines with longer half-lives provide smoother blood pressure control – e.g. chronic hypertension
Cardiac Dysrhythmias • Treated mainly with verapamil and diltiazem • Management of: • Supraventricular tachycardias • atrial fibrillation • Result in a decrease in SA node pacemaker rate and AV node conduction • Block at the AV node, thus decreasing impulses into the ventricles –e.g. atrial fibrillation
Angina pectoris • Chest pain due to ischemia of the heart muscle • Oxygen supply to the heart does not meet oxygen demand • Caused by obstruction or spasm of the coronary arteries (oxygenated blood to the heart), harder to supply blood to the heart • Reduction of oxygen demand • Decrease afterload • Decrease heart rate • Decrease contractile force Block entry L-type Ca2+ channel
Side effects and toxicity • Most common: constipation, nausea, headache, edema, dizziness, sexual dysfunction • More severe: liver dysfunction, gum hypertrophy • Symptoms of heart failure may worsen due to the reduced ability for the heart to pump blood • Excessive inhibition of Ca2+ channel blockage may induce cardiac depression such as cardiac arrest, bradycardia, atrioventricular block, and heart failure
summary • Activation of Voltage-Gated Calcium Channels directly increase Cytosolic [Ca+2] in cardiac muscle and indirectly increase [Ca+2] by activating calcium-dependent calcium release via Ryanodine Receptor Channel • Voltage-Gated Calcium Channels prolong the AP in cardiac muscle cells • CCB’s act on L-type calcium channels by acting on the alpha-1 subunit • CCB’s used to treat cardiovascular disease include the dihydropyridine family and non-dihydropyridines (e.g. Verapimil & Diltiazem) • Antihypertensives act by Inhibiting calcium influx into arterial smooth muscle cells • Verapimil and diltiazem are used in the management of supraventricular tachycardias and atrial fibrillation by decreasing SA and AV node conduction • Angina • Heart’s oxygen supply < Heart’s oxygen demand • Treatment: reduce oxygen demand by blocking L-type Ca2+ channel • Excessive inhibition of L-type Ca2+ channel may lead cardiac arrest and heart attack
references • Basic and Clinical Pharmacology. • Calcium Channel Blockers (CCBs) <http://www.medicinenet.com/calcium_channel_blockers/article.htm> • Koschak A, Reimer D, Huber I, Grabner M, Glossmann H, Engel J, et al. alpha 1D (Cav1.3) subunits can form l-type calcium channels activating at negative voltages. J BiolChem 2001; 276:22100-6. • Morgans CW, Gaughwin P, Maleszka R. Expression of the alpha1F calcium channel subunit by photoreceptors in the rat retina. Mol Vis 2001; 7:202-9. • Munther K, Hormoud MD, 2007 Monophasic Acition Potential (Cardiac Muscle Cell) • Samarasinghe Y P, Cox A, Fehers MD. Calcium channel blocker induced gum hypertrophy: no class distinction. <http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1768009/> • Tanabe T, Beam KG, Adams BA, Niidome T, Numa S. Regions of the skeletal muscle dihydropyridine receptor critical for excitation-contraction coupling. Nature 1990; 346:567-569.