Download
1 / 121
1.25k likes | 1.72k Vues
Injuries of the Clavicle, Acromioclavicular Joint and Sternoclavicular Joint. Andrew H. Schmidt, M.D. Revised October 2010 Andrew H. Schmidt, MD & T. J. McElroy, MD; Created March 2004; Revised January 2007 & October 2010. Goals.

E N D
Injuries of the Clavicle, Acromioclavicular Joint and Sternoclavicular Joint Andrew H. Schmidt, M.D. Revised October 2010Andrew H. Schmidt, MD & T. J. McElroy, MD; Created March 2004; Revised January 2007 & October 2010
Goals • 1) Review anatomy of clavicle, AC joint, and sternoclavicular joint • 2) Review imaging of these areas. • 3) Clavicle Fractures Nonoperative RX Surgical Repair Nonunions and Malunions • 4) AC Joint Injuries • 5) Sternoclavicular joint injuries
Clavicle • “S”-shaped bone • Medial - sternoclavicular joint • Lateral - acromioclavicular joint and coracoclavicular ligaments • Muscle attachments: • Medial: sternocleidomastoid • Lateral: Trapezius, pectoralis major
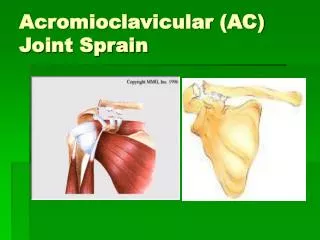
AC Joint • Diarthrodial joint between medial facet of acromion and the lateral (distal) clavicle. • Contains intra-articular disk of variable size. • Thin capsule stabilized by ligaments on all sides: • AC ligaments control horizontal (anteroposterior ) displacement • Superior AC ligament most important
Distal Clavicle • Coracoclavicular ligaments • “Suspensory ligaments of the upper extremity” • Two components: • Trapezoid • Conoid • Stronger than AC ligaments • Provide vertical stability to AC joint
Mechanism of Injury • Direct impact to the anterior - superior shoulder of moderate – high force. • Fall from height • Motor vehicle accident • Sports injury • Blow to the point of the shoulder • Rarely, a direct injury to the clavicle
Physical Examination • Inspection • Evaluate deformity and/or displacement • Beware of rare inferior or posterior displacement of distal or medial ends of clavicle • Compare to opposite side.
Physical Examination • Palpation Evaluate pain Look for instability with stress
Physical Examination • Neurovascular examination • Must be done thoroughly and documented! • Evaluate upper extremity motor and sensation • Measure shoulder range-of-motion
Radiographic Evaluationof the Clavicle • Anteroposterior View • 30-degree Cephalic Tilt View
Radiographic Evaluation of the Clavicle • Quesana View • 45-degree angle superiorly and a 45-degree angle inferiorly • Provide better assessment of the extent of displacement
Radiographic Evaluation of the AC Joint • Zanca View • AP view centered at AC joint with 10 degree cephalic tilt • Less voltage than used for AP shoulder
Stress Views of the Distal Clavicle & AC Joint • Rationale: demonstrate instability and differentiate grade III AC separations from partial Grade I-II injuries. • Performed by having patient hold 10# weight with injured arm. • Rarely used today, since most Grade I-III AC joint injuries are treated the same anyway, and management of distal clavicle fractures depends on initial displacement and location of fracture.
Radiographic Evaluation of the Medial One Third • X-ray: Cephalic tilt view of 40 to 45 degrees • CT scan usually indicated to best assess degree and direction of displacement S=sternum C= medial clavicle E= esophagus
Classification of Clavicle Fractures • Group I : Middle third • Most common (80% of clavicle fractures) • Group II: Distal third • 10-15% of clavicle injuries • Group III: Medial third • Least common (approx. 5%)
Treatment Options • Nonoperative • Sling • Brace • Surgical • Plate Fixation • Screw or Pin Fixation • Titanium elastic nails (usually inserted medial to lateral)
Nonoperative Treatment • “Standard of Care” for most clavicle fractures. • Unclear about the need to wear a specialized brace.
Simple Sling vs. Figure-of-8 Bandage • Prospective randomized trial of 61 patients • Simple sling • Less discomfort • Functional and cosmetic results identical • Alignment of healed fractures unchanged from the initial displacement in both groups Andersen et al., Acta Orthop Scand 58: 71-4, 1987.
Nonoperative Treatment • It is difficult to reduce clavicle fractures by closed means. • Most clavicle fractures unite rapidly despite displacement. • Significantly displaced mid-shaft and distal-third injuries have a higher incidence of nonunion.
Nonoperative Treatment • There is new evidence that the outcome of nonoperative management of displaced middle-third clavicle fractures is not as good as traditionally thought, with many patients having significant functional problems.
Deficits following nonoperative treatment of displaced midshaft clavicular fractures • A patient-based outcome questionnaire and muscle-strength testing were used to evaluate 30 patients after nonoperative care of a displaced midshaft fracture of the clavicle. • At a minimum of twelve months (mean 55 mos), outcomes were measured with the Constant shoulder score and the DASH patient questionnaire. In addition, shoulder muscle-strength testing was performed with the Baltimore Therapeutic Equipment Work Simulator, with the uninjured arm serving as a control. McKee et al. J Bone Joint Surg Am 2006;88-A:35-40.
Deficits following nonoperative treatment of displaced midshaft clavicular fractures • The strength of the injured shoulder was: • 81% for maximum flexion, 75% for endurance of flexion, • 82% for maximum abduction, 67% for endurance of abduction, • 81% for maximum external rotation, 82% for endurance of external rotation, • 85% for maximum internal rotation, and 78% for endurance of internal rotation (p < 0.05 for all). • Mean Constant score = 71 points • Mean DASH score = 24.6 points, indicating substantial residual disability. McKee et al. J Bone Joint Surg Am 2006;88-A:35-40.
Conclusion of McKee study • Displaced midshaft clavicle fractures can cause significant, persistent disability, even if they heal uneventfully.
Definite Indications for Surgical Treatment of Clavicle Fractures • 1) Open fractures • 2) Associated neurovascular injury
Relative Indications for Acute Treatment of Clavicle Fractures • 1) Widely displaced fractures • 2) Multiple trauma • 3) Displaced distal-third fractures
Relative Indications for Acute Treatment of Clavicle Fractures • 4) Floating shoulder • 5) Seizure disorder • 6) Cosmetic deformity • 7) Earlier return to work.
ClavicularDisplacement Literature • < 5 mm shortening: acceptable results at 5 years (Nordqvist et al, Acta Orthop Scand 1997;68:349-51. • > 20 mm shortening associated with increased risk of nonunion and poor functional outcome at 3 years (Hill et al, JBJS 1997;79B: 537-9)
Plate Fixation • Traditional means of ORIF • Plate applied superiorly or inferiorly Inferior plating associated with lower risk of hardware prominence. • Used for acute displaced fractures and nonunions.
May dissect out supraclavicular sensory nerves Courtesy T. Higgins
Nonoperative Treatment Compared with Plate Fixation of Displaced Midshaft Clavicular Fractures. A multicenter, randomized clinical trial • 132 patients • 67 ORIF • 65 sling • Constant and DASH scores significantly improved in ORIF group. • Time to union 16 vs 28 weeks in favor of ORIF • 9 patients in sling group had symptomatic malunion • 9 patients in ORIF group had hardware complications Canadian Orthopedic Trauma Society; JBJS Am;2007:89A: 1-10
Intramedullary Fixation • Large threaded cannulated screws • Flexible elastic nails • K-wires Associated with risk of migration • Useful when plate fixation contra-indicated Bad skin Severe osteopenia • Fixation less secure
Titanium Elastic Nails • Same as used in pediatric femur fractures. • Accommodate three-dimensional anatomy of the clavicle. • Typically inserted “retrograde” (from medial to lateral) • Best in fractures without comminution • Small incision at fracture site may be needed.
Minimally Invasive Intramedullary Nailing of MidshaftClavicular Fractures Using Titanium Elastic Nails • 31 cases evaluated 26 mos avg (6-46 mos) • Three groups: Isolated, n=9 Additional injuries, n=15 Multiple injuries, n=7 Mueller M, et al. J Trauma 2008;64:1528-1534
Minimally Invasive Intramedullary Nailing of MidshaftClavicular Fractures Using Titanium Elastic Nails • No nonunions or refractures in any group. • 7 cases medial migration; 1 case lateral perforation in 1 case req’d shortening of nail. • No differences in outcome between groups in subjective outcome and objective scores (DASH, Constant and Murley). Mueller M, et al. J Trauma 2008;64:1528-1534
30 patients elastic nail 100% union 7 cases medial nail protrusion 2 refractures Better DASH and Constant outcome scores, significantly different during first 18 weeks. Patients more satisfied with cosmetic appearance and overall outcome. • 30 patients: simple shoulder sling • 90% union • 2 symptomatic malunions req’d OR
Comparison of Techniques • No studies available that compare one operative technique to another. • Both elastic nails and plates seem equivalent in stable fractures; benefits of minimally invasive approach used in elastic nailing awaiting study. • Plate fixation best in comminuted fractures, but again no evidence.
Does Timing of Surgery Matter? • Matched group comparison of 15 patients who underwent early compression plate fixation to 15 other patients who had operative repair of a malunion/nonunion at avg of 63 months. Potter JM, et al. J Shoulder Elbow Surg 2007;16:514-8
Does Timing of Surgery Matter? • OutcomeEarly Delayed • Strength = = • Endurance 109% 80% (p=.05) • Constant score 95 89 (p=.02) • DASH score 3.0 7.2 (p=.15) • Satisfaction exc exc Potter JM, et al. J Shoulder Elbow Surg 2007;16:514-8
Does Timing of Surgery Matter? • Conclusion: Late reconstruction provides outcome similar to acute repair, except for subtle decreases in endurance strength. • Such information might be of value in initial decision-making. Potter JM, et al. J Shoulder Elbow Surg 2007;16:514-8
Complications of Clavicular Fractures and its Treatment • Nonunion • Malunion • Neurovascular Sequelae • Post-Traumatic Arthritis
Risk Factors for the Development of Clavicular Nonunions • Location of Fracture • (outer third) • Degree of Displacement • (marked displacement) • Primary Open Reduction
Principles for the Treatment of Clavicular Nonunions • Restore length of clavicle • May need intercalary bone graft • Rigid internal fixation, usually with a plate • Iliac crest bone graft • Role of bone-graft substitutes not yet defined.