Atrial Fibrillation
Atrial Fibrillation. Outline. Epidemiology Signs and Symptoms Etiology Differential Diagnosis Diagnostic Tests Classification Management. Epidemiology. Most frequently diagnosed arrhythmia Affects 2.3 million people in the US Affects 1/136 people in the US


Atrial Fibrillation
E N D
Presentation Transcript
Outline • Epidemiology • Signs and Symptoms • Etiology • Differential Diagnosis • Diagnostic Tests • Classification • Management
Epidemiology • Most frequently diagnosed arrhythmia • Affects 2.3 million people in the US • Affects 1/136 people in the US • Columbus population 769,360 (2009) • Would expect to see 5600 pts/year! • Incidence increases with age
Signs and Symptoms • Palpitations • Weakness • Dizziness • Reduced exercise capacity • Dyspnea • Asymptomatic
Etiology/Risk Factors • Structural heart disease • Chronic lung disease • Pneumonia • Hyperthyroidism • Alcohol use • Pulmonary embolism • HTN • Pericarditis Key Point MI is a very rare cause of Afib! Think twice before doing a ROMI
Differential Diagnosis • Narrow Complex Tachycardias • Atrial Fibrillation • Atrial Flutter • AVNRT • AVRT • Atrial tachycardia • Sinus tachycardia • Multifocal atrial tachycardia SVT is a category, not a diagnosis!
Classification • Paroxysmal: terminates in < 7 days • Persistent: fails to terminate within 7 days • Permanent: > 1 year • Lone: Individuals without structural heart disease, < 60 yrs old
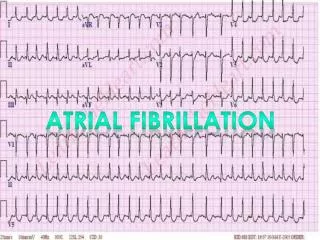
Diagnostic Testing: EKG Irregularly Irregular Narrow Complex Rapid Ventricular Rate
Diagnostic Testing: TTE • To assess for structural heart disease • EF • Wall motion • Dilation/Hypertrophy • Size of right and left atrium • Valvular disease • Pericardial disease
Chest X-Ray • Look for emphasema/COPD • Cardiac borders • Pneumonia Rush Center for Congenital and Structural Heart Disease
Management • Rate Control • Rhythm Control • Anticoagulation • Unstable patients
Rate Control • Why is rate control important? • Ischemia, MI, hypotension can occur • Long term: Cardiomyopathy • Goals • Rest HR < 80 bpm • 24 Hour (Tele/Holter) < 100 bpm average • HR < 110 in 6 minute walk Key Point
Rate Control (con’t) • Medications • Metoprolol / Esmolol: IV or Oral • Diltiazem: IV or Oral • Verapamil: Oral Only • Digoxin: Patients with hypotension • Amiodarone: Also for rhythm control
Rhythm Control • Indications • Symptoms of a-fib persistent • To avoid long term anticoagulation • Bleeding risk • Personal preferenance
Rhythm Control (con’t) • Synchronized DC cardioversion • Emergencies/Hemodynamic instability • Greater efficacy than medications • Pharmacologic cardioversion • If AF < 7days – dofetilide, flecainide, ibutilide, propaferone or amiodarone • If AF > 7 day – dofetilide or amiodarone
Rate or Rhythm Control? • Affirm Study: Rate versus rhythm control • No difference in incidence of stroke • Trend towards lower mortality in the rate control group • See article • This is STILL a controversial topic!
Anticoagulation and Cardioversion • Afib < 48 hours: • Cardioversion (CV) • No anticoagulation indicated • Afib > 48 hours: • Anticoagulate for 3-4 weeks before CV • OR get TEE • Anticoagulate for 1 month after CV
Anticoagulation – Long Term • Risk of CVA determined by CHADS2 score (CHF, HTN, >75, DM, Previous CVA x 2) Key Points Most patients, can wait 48 hours before starting 0-1 probably don’t need anticoagulation 5-6 should be bridged with heparin/LMWH
Management – Unstable Key Point Unstable: A-fib associated with Hypotension Synchronized electric Cardioversion immediately
Key Points • MI is a rare CAUSE of a-fib • Rate control must be achieved during exercise, not just at rest • Not every patients needs to bridge with heparin • Unstable patients should immediately be cardioverted