Download
1 / 23
230 likes | 442 Vues
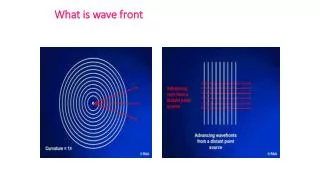
What is Real and What is Not. A Third Wave Approach to Formulating Psychosis . Isabel Clarke and Donna Rutherford Clinical Psychologists New Forest & TVS: AOT, Inpatient and CRHT. “Third Wave” Cognitive Therapies. Developments in CBT as it tackles personality disorder, psychosis etc.

E N D
What is Real and What is Not. A Third Wave Approach to Formulating Psychosis Isabel Clarke and Donna Rutherford Clinical Psychologists New Forest & TVS: AOT, Inpatient and CRHT.
“Third Wave” Cognitive Therapies • Developments in CBT as it tackles personality disorder, psychosis etc. • Therapeutic relationship important • Past history is significant • Change lies not so much in altering thought to alter feeling, but in altering the person’s relationship to both thought and feeling • Mindfulness is a key component. • Recognition of a split or incompleteness in human cognition – which mindfulness can bridge.
“Third Wave” – term coined by Hayes (Acceptance & Commitment Therapy) • Kabat-Zinn. Applied mindfulness to stress and pain. • Segal, Teasdale & Williams. Mindfulness Based Cognitive Therapy (relapse in depression.) • Linehan. Dialectical Behaviour Therapy (BPD) • Chadwick. Mindfulness groups for voices. • Hayes
LEVELS OF PROCESSING – A THEORETICAL JUNGLE! • First wave CBT comes unstuck over the gap between logical reasoning and strong emotion. This leads to the recognition of different types or levels of processing. e.g.s of theories of this. • Ellis: Inference and Evaluation • Hot and Cold cognition • Power & Dalgleish. SPAARS (theory of emotion). • Mark Williams: overgeneral autobiographical memory. • Metacognition. • Wells & Mathews. S-REF • Brewin’s VAMS and SAMS (just memory). • Ehlers & Clark (following Roediger): conceptual v.data driven processing. • Perceptual Control Theory and the Method of Levels. • AND INTERACTING COGNITIVE SUBSYSTEMS!
Features the theories have in common. • All suggest 2 or more separate types of processing – the split in human cognition! • There is one direct, sensory driven, type of processing and a more elaborate and conceptual one. • The same distinction can be found in the memory. • Direct processing is emotional and characteristed by high arousal. • This is the one that causes problems – e.g. flashbacks in PTSD. • The two central meaning making systems of ICS provides a neat way of making sense of this.
DIALECTICAL BEHAVIOUR THERAPY: Linehan’s STATES OF MIND EMOTION MIND REASONABLE MIND WISE MIND IN THE PRESENT IN CONTROL
Interacting Cognitive Subsystems. Body State subsystem Implicational subsystem Auditory ss. Implicational Memory Visual ss. Verbal ss. Propositional subsystem Propositional Memory
A challenging model of the mind. • There is no boss – our unitary sense of self is an illusion! • The mind is simultaneously individual, and reaches beyond the individual, when the implicational ss. is dominant. • This happens at high and at low arousal. • There is a constant balancing act between logic and emotion – human fallibility • Dysynchrony between the systems explains anomalous experiences – psychosis! • Mindfulness is a useful technique to manage the balance.
Taking Experience Seriously in Psychosis • Acknowledging that psychosis feels different • Normalising the difference as well as the continuity • Sensitivity and openness to anomalous experience – continuum with normality: Gordon Claridge’s Schizotypy research. • Understanding the role of emotion – where expression of emotion is not straightforward.
2 Ways of experiencing • ICS gives us a normalizing way of understanding the experience of difference. • When the imp.ss and the prop.ss are working together, that gives us an ordinary, grounded quality of experience. • When they become desynchronized, the imp. temporarily takes over • This feels different; in extreme forms leads to openness to anomalous experience. • This quality of experience is also sought and valued!
Ordinary Clear limits Access to full memory and learning Precise meanings available Separation between people Clear sense of self Emotions moderated and grounded Logic of Either/Or Supernatural Unbounded Access to propositional knowledge/memory is patchy Suffused with meaning or meaningless Self: lost in the whole or supremely important Emotions: swing between extremes or absent Logic of Both/And Shared Reality Unshared Reality
Evidence for a new normalisation • Schizotypy – a dimension of experience: Gordon Claridge. • Mike Jackson’s research on the overlap between psychotic and spiritual experience. • Emmanuelle Peter’s research on New Religious Movements. • Caroline Brett’s research: having a context for anomalous experiences makes the difference between whether they become diagnosable mental health difficulties • and whether the anomalies/symptoms are short lived or persist. • Wider sources of evidence – e.g.Cross cultural perspectives; anthropology. Richard Warner: Recovery from Schizophrenia.
Being Porous: therapeutic approach • Some people are more open to this type of experience than others – cf. Schizotypy • People high on the schizotypy spectrum are more sensitive and “open”. • Leading to the need to regulate stimulation. • This can lead into an avoidance cycle; social isolation and withdrawal = psychotic reality takes over. • Sensitivity and openness to anomolous experience – continuum with normality • Positive side as well as vulnerability
Normalising the difference in quality of experience as well as the continuity • Validating the person’s experience • Helping people to manage the threshold – mindfulness is key Understanding the role of emotion and arousal – the feeling is real, though the story might be suspect. • All this helps with building a therapeutic alliance. • Persuasion to join “shared reality” – motivational work. Realistic about the risks of “unshared reality”. • Recognizing the attraction of “unshared reality” for many – offering specialness, buzz and a handy escape • Mobilising and nurturing strengths • Creative expression
Helping someone get their bearings by mapping the 2 states. • These sorts of experiences can be very confusing and disorienting – it helps it someone can come up with a map. • Explain that there are 2 states, and some people are more open than others • Find a way of describing this that works for your client (e.g. ‘Your Reality’ and ‘Shared Reality’ • Draw out two columns • Sort out the person’s story into the two – being very tactful where you are suggesting that it lies in the non-shared side – hint: Non-shared reality has a ‘both-and’ logic – 2 incompatible things can be true at the same time! • This can be used as a framework for future sessions.
What is real & what is not?: about the programme. • A 4 session group programme for an Acute inpatient setting. • Run by a clinical psychologist and one or two others – trainees, nurses, OT etc. • Builds on the Romme and Escher ‘Voices Group’ tradition • Is different from other CBT approaches in normalizing the difference in quality of experience in psychosis, as well as thinking style. • This normalization attacks stigma by associating psychosis with valued areas such as creativity and spirituality. • Attempts to mitigate the damage to self concept of the traditional, diagnosis, based approach.
Therapeutic Alliance • As this approach represents a new normalisation, it can greatly aid the therapeutic alliance • The individual’s experience is taken seriously and valued – at the same time as working on a better relationship to shared experience • It is possible to get away from illness language – and arguments about diagnosis • The schizotypy continuum is a good normaliser – association of high s. with creativity etc.
The group programme: Session 1. • Introduce Romme and Escher • Extending from voices to other experiences that people in general do not share. • Idea of openness to voices and strange experiences. Schizotypy spectrum. Artists etc. David Bowie example. • Examples from the group – what do they want to get out of the sessions. Fill in goal form.
Session 2. The role of Arousalshaded area = anomalous experience/symptoms are more accessible. HighArousal - stress
Session 2 cont. DIALECTICAL BEHAVIOUR THERAPY: Linehan’s STATES OF MIND applied to PSYCHOSIS Discussion of Ways of coping suggested by this approach – management of arousal and distraction.
Session 3: mindfulness & 4: making sense. • Introducing Focussing. Haddock research on Focussing and Distraction. • Mindfulness and focussing. • Mindfulness exercise. • ****************************************How do people make sense of their experiences? Disussion of different ways of making sense of them. • Clue: what was happening when they first started? • Feedback, summing up and completing the goal sheet again.
The Challenge of Evaluation in the Inpatient Setting • People in crisis are not keen to fill in a lot of questionnaires – and are not very good at it. • Even with only 4 sessions, consistency of attendance and retention are a problem • A CSIP grant enabled us to employ an assistant one day a week for 6 months. • She used CORE, Mental Health Confidence Scale and a specially designed exit questionnaire, as well as the goal setting measure which is integral to the group. • Encouraging results (only before and after measures) • We have just submitted the paper to Clinical Psychology and Psychotherapy – wish us luck!
Contact details, References and Web address • Isabel.Clarke@hantspt-sw.nhs.uk • Donna.Rutherford@hantspt-sw.nhs.uk • AMH Woodhaven, Calmore, Totton SO40 2TA. • Clarke, I. & Wilson, H.Eds. (2008)Cognitive Behaviour Therapy for Acute Inpatient Mental Health Units; working with clients, staff and the milieu. London: Routledge. • Clarke, I. ( 2008) Madness, Mystery and the Survival of God. Winchester:'O'Books. • Clarke, I. (Ed.) (2001) Psychosis and Spirituality: exploring the new frontier. Chichester: Wiley • Durrant, C., Clarke, I., Tolland, A. & Wilson, H. (2007) Designing a CBT Service for an Acute In-patient Setting: A pilotevaluation study. Clinical Psychology and Psychotherapy. 14, 117-125. • www.isabelclarke.org