Continence Management
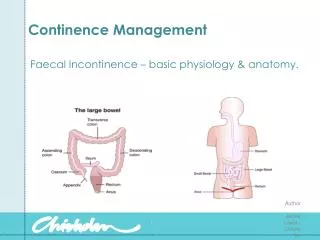
Continence Management. Faecal Incontinence – basic physiology & anatomy. Continence Management. A normal bowel : Can vary greatly in frequency – from 3 times a day to once every three days. Will form soft motions. Should not have to strain to empty.

Continence Management
E N D
Presentation Transcript
Continence Management • Faecal Incontinence – basic physiology & anatomy. Author - Jackie Laver - Chisholm 2009
Continence Management • A normal bowel : • Can vary greatly in frequency – from 3 times a day to once every three days. • Will form soft motions. • Should not have to strain to empty. • Should not experience any accidental loss of faeces. • Should not take longer than a minute to fully evacuate. • Should not experience any pain when emptying. Author - Jackie Laver - Chisholm 2009
Continence Management • * It is estimated approximately 275,000 people in Australia suffer from faecal incontinence. • * It is NOT a normal part of ageing or from giving birth. • * Around 50% of people with incontinence never seek help. Author - Jackie Laver - Chisholm 2009
Continence Management • * Faeces – consists of a semi-solid brown mass, made up of 60-70% water, fibre, indigestible cellular plant and animal matter, dead & live microbes, enzymes, epithelial cells, mucus, bile & fatty acids. • * Defaecation occurs as a result of the peristaltic movements of the intestines pushing the faeces into the rectum. As the rectum begins to stretch, it sends impulses to our brains which registers this sensation. • * We then go to the toilet! Author - Jackie Laver - Chisholm 2009
Continence Management • Bowel habits can be altered because of: • Age – Peristalsis reduces with age. • Personal habits – privacy! This is a very private thing. Odours and noise can lead to embarrassment, and if the urge to defaecate is suppressed, this can lead to constipation and distension. • Diet – a diet high in fibre will increase the peristalsis, and softens and adds weight to the stool. • Fluid intake – the weight of faeces is 60-70% water. Dehydration causes hard faeces which is difficult & painful to pass. The elderly are often chronically dehydrated. • Physical activity – this promotes peristalsis. Inactivity decreases bowel motility. • Pain – anal fissures or haemorrhoids may cause pain, and so reluctance to defaecate may develop. • Psychology – anxiety & stress can lead to increased motility and diarrhoea. Depression can lead to decreased motility and constipation. Author - Jackie Laver - Chisholm 2009
Continence Management • Pregnancy – the weight of the growing foetus can exert pressure on the bowel, impeding the movement of the faeces through the bowel. • Surgery – any bowel surgery can temporarily reduce or cease peristalsis. • Disease – Ulcerative colitis, Crohn’s disease, diverticulitis, bacterial infection – eg, salmonella, Rota virus. • Medication – • over use of laxatives (very common in the past) can lead to reduced bowel tone and the inability to respond to normal stimulation. • Narcotics (eg. Codiene or morphine) slow peristalsis. • Antibiotics alter the normal flora in the bowel, and can lead to bowel irritability and increased motility. • NSAID’s – also lead to bowel irritability. Author - Jackie Laver - Chisholm 2009
Continence Management • Types of Faecal Incontinence – basically the same as for urinary incontinence. • 1. Stress. • 2. Urge. • 3. Overflow. • 4. Functional. • 5. Reflex. Author - Jackie Laver - Chisholm 2009
Continence Management • Dementia & bowel control – people with dementia may have trouble with : • ‘Holding on’ until they get to a toilet • Finding a toilet • Knowing how to undress at the toilet • Knowing when their bladder or bowel is empty. • Being aware when they need to empty their bladder or bowels. • Going to the toilet in inappropriate places. • Anxiety, stress or depression – which may make their toileting more difficult. Author - Jackie Laver - Chisholm 2009
Continence Management • Diarrhoea – the frequent discharge of loose unformed stools. • Causes – • Irritation or inflammation of the GI tract – due to infection, medications or highly spiced foods. • Disease – ulcerative colitis, Crohn’s disease, diverticulitis, IBS, diabetes (neuropathy). • Disorders of digestion or absorption – eg. Coeliac, dairy intolerance. • Disorders that affect the secretion of digestive fluids – eg. Obstructive jaundice. • Medications – too many laxatives, antibiotics. • Anxiety or stress. • Can happen as a result of constipation – impaction with overflow. Author - Jackie Laver - Chisholm 2009
Continence Management • Constipation – the passage of hard dry stools, unrelated to frequency. • Caused by – • lack of fibre, water or mobility +/- activity. • Chronic use of laxatives. • Certain disease states – Parkinson’s, CVA, MS. • Avoiding the need to defaecate. • Some medications – eg. Iron tablets, codeine • Bowel disease – haemorrhoids, IBS, diverticulitis. Often accompanied by : abdominal distention & bloating, nausea, headache, anorexia. Author - Jackie Laver - Chisholm 2009
Faecal Impaction • Faecal impaction results from prolonged exposure of stool to the absorptive process of the colon and rectum. • As a result of this, the stool can become extremely hard. It is important to note that faecal impaction may present as diarrhoea, and that impaction may not be detected during rectal examination. Author - Jackie Laver - Chisholm 2009
Continence Management Author - Jackie Laver - Chisholm 2009
Successful bowel management involves responding to issues • Identification of any health problems or symptoms or potential health problems e.g. Pain, bleeding or discomfort on motion, haemorrhoids, agitation, confusion, • Identification of dietary or medications needs. These will have been identified as a result of bowel assessment and documented in the Care Plan and may include: the need for additional fruit, fruit juice, and extra fluids to keep the bowels open regularly, the need for aperients, stool softeners or fibre supplements, or the need for suppositories • Identification of a range of individual support strategies. These may include, exercise to stimulate peristalsis, abdominal massage, or the need for continence pads • Identification of problems associated with faecal incontinence. Indicators may include, frequent soiling underwear, hiding underwear, faecal smearing. Author - Jackie Laver - Chisholm 2009
Continence Management • Faecal incontinence – Principles of management. • 1. Identify the cause and treat appropriately. • 2. The person’s hygiene needs must be attended to, and • 3. Maintain dignity & self esteem. Author - Jackie Laver - Chisholm 2009
Continence Management • Diarrhoea : • Cause – infection • Treatment – virus – time, bacterial – antibiotics. • Cause – UC, Crohn’s, diverticulitis, IBS. • Treatment – low irritant diet, reduce stress. • Management – pads, easy access to toilet. • Cause - Food intolerances, eg, Coeliac, dairy. • Treatment – remove irritants from diet. Author - Jackie Laver - Chisholm 2009
Continence Management • Constipation : • Cause – dietary – lack of fibre, water. • Treatment – improve diet. • Cause - Chronic use of laxatives. • Treatment – bowel regime. • Cause – some medications – eg. codiene. • Treatment – look for alternatives, or use regular laxatives. Author - Jackie Laver - Chisholm 2009
Continence Management • Promoting Continence : • Treat the cause. • Ensure good hygiene & skin care. • Ensure adequate hydration. • Promote healthy diet with fruit, vegies, whole grain bread. Use fibre supplements if needed – eg. Benefibre. • Ensure adequate access to toilets – good lighting, wide doors, close to group areas and dining rooms. • Use commodes or urinals if appropriate. • Manage privacy & dignity of client. • Ensure clothes are easily removed. • Adhere to toileting schedules. Author - Jackie Laver - Chisholm 2009
Bowel Assessment • What is a normal bowel pattern? • Any recent changes in their bowel habits? • Frequency of bowel movements • The consistency of the stool • Their normal activities to maintain bowel function (e.g. what works for them) • The presence of faecal/urinary incontinence • The need for frequent straining during toileting • If recent illness (e.g. stroke), what wads their normal bowel pattern prior to the illness • What, if any, laxatives are being taken, the type, frequency and length of time of use • The person’s preferences and special toileting needs, e.g. Privacy, raised foot stool, raised toilet seat. Author - Jackie Laver - Chisholm 2009
Continence Assessment • Presenting Problem – • Urinary / faecal a. stress b. urge c. overflow d. functional e. reflex Author - Jackie Laver - Chisholm 2009
Continence Assessment • 2. Relevant diagnosis – • a. CVA • b. dementia • c. spina bifida • d. diabetes • e. Parkinson’s disease Author - Jackie Laver - Chisholm 2009
Continence Assessment • 3. Gynae / urological history – • a. prostatectomy • b. multiple pregnancies • c. atrophic vagina / urethra • d. hysterectomy Author - Jackie Laver - Chisholm 2009
Continence Assessment • 4. Previous investigations – • 1. MSU • 2. urinalysis • 3. bladder scan • 4. urodynamics • 5. IVP Author - Jackie Laver - Chisholm 2009
Continence Assessment • 5. Psychosocial effects – • 1. embarrassed • 2. withdrawn • 3. apathetic • 4. denial • 5. depression Author - Jackie Laver - Chisholm 2009
Continence Assessment • 6. Self awareness – • * is resident aware of incontinence? • * what insight is the patient demonstrating? Author - Jackie Laver - Chisholm 2009
Continence Assessment • 7. Communication – • a. ability to request toileting • b. familiar terms used • c. language difficulties • d. cognitive ability Author - Jackie Laver - Chisholm 2009
Continence Assessment • 8. Behavioural Cues – • - when patient wants to void / defaecate, he / she - • 1. becomes restless • 2. becomes verbally agitated • 3. wanders Author - Jackie Laver - Chisholm 2009
Continence Assessment • 9. Coping strategies – • 1. regular toileting • 2. use of tissues / pads • 3. fluid reduction Author - Jackie Laver - Chisholm 2009
Continence Assessment • 10. Environmental – • 1. location of toilets • 2. raised seat • 3. commode • 4. clothing – belts, buckles, buttons, stockings. Author - Jackie Laver - Chisholm 2009
3 day assessment Author - Jackie Laver - Chisholm 2009
References: • www.continence.org.au • www.bladderbowel.gov.au • Scott, K., Webb, M., Sorrentino, S. & Gorek, B. “Long Term Care Assisting”, Elsevier, Marrickville, NSW. 2007. • Funnel, R., Koutoukidis, G., Lawrence, K. “Tabbner’s Nursing Care – 4E” Elsevier, Marrickville, NSW. 2005. Author - Jackie Laver - Chisholm 2009